

Multicenter Canadian study of prehospital trauma care
- PMID: 12560770
- PMCID: PMC1522139
- DOI: 10.1097/01.SLA.0000048374.46952.10
Multicenter Canadian study of prehospital trauma care
Abstract
Objective: To evaluate whether the type of on-site care a trauma patient receives affects outcome.
Summary background data: The controversy regarding the prehospital care of trauma patients between Advanced Life Support (ALS) and Basic Life Support (BLS) is ongoing. Due to this unresolved controversy, as well as historical, cultural, and political factors, there are significant variations with respect to the type of prehospital care available for trauma patients.
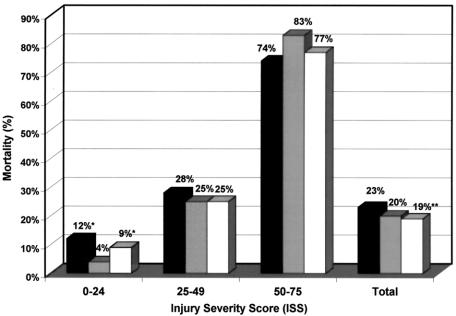
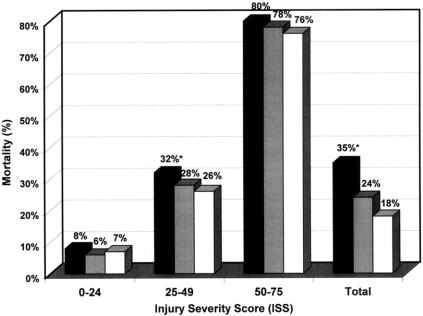
Methods: This prospective cohort study compared three types of prehospital trauma care systems: Montreal, where physicians provide ALS (MD-ALS); Toronto, where paramedics provide ALS (PMD-ALS); and Quebec City, where emergency medical technicians provide BLS only (EMT-BLS). The study took advantage of this variation to evaluate the association between the type of on-site care and mortality in patients with major life-threatening injuries. All patients were treated at highly specialized tertiary (level I) trauma hospitals. The main outcome measure was death as a result of injury. Follow-up was to hospital discharge.
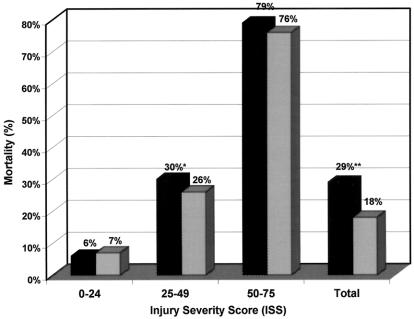
Results: The overall mortality rates by type of on-site personnel were physicians 35%, paramedics 24%, and EMTs 18%. For patients with major but survivable trauma, the overall mortality rates were physicians 32%, paramedics 28%, and EMTs 26%. The overall mortality rate of patients receiving only BLS at the scene was 18% compared to 29% for patients receiving ALS. For the subgroup of patients with major but survivable injuries, the mortality rates were 30% for ALS and 26% for BLS. The adjusted increased risk for mortality in patients receiving ALS at the scene was 21%.
Conclusions: In urban centers with highly specialized level I trauma centers, there is no benefit in having on-site ALS for the prehospital management of trauma patients.
Figures
Comment in
-
Prehospital care: do no harm?Ann Surg. 2003 Feb;237(2):161-2. doi: 10.1097/01.SLA.0000048440.07546.45. Ann Surg. 2003. PMID: 12560771 Free PMC article. No abstract available.
References
-
- Health Reports. Canadian Centre for Health Information. Statistics Canada, Ottawa, 1989.
-
- Mortality. Summary List of Causes, Vital Statistics. Health Division, Vital Statistics and Health Status Section, Statistics Canada, Ottawa, 1987–1990.
-
- Health Reports. Statistics Canada. Vol. 7, No. 1, Cat. No. 82–003, 1995.
-
- Hedges JR, Sacco WJ, Champion HR. An analysis of prehospital care of blunt trauma. J Trauma 1982; 22: 989–993. - PubMed
-
- Aprahamian C, Thompson BM, Towne JB, et al. The effect of a paramedic system on mortality of major open intra-abdominal vascular trauma. J Trauma 1983; 23: 687–690. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
