

HIV protease inhibitors promote atherosclerotic lesion formation independent of dyslipidemia by increasing CD36-dependent cholesteryl ester accumulation in macrophages
- PMID: 12569165
- PMCID: PMC151854
- DOI: 10.1172/JCI16261
HIV protease inhibitors promote atherosclerotic lesion formation independent of dyslipidemia by increasing CD36-dependent cholesteryl ester accumulation in macrophages
Abstract
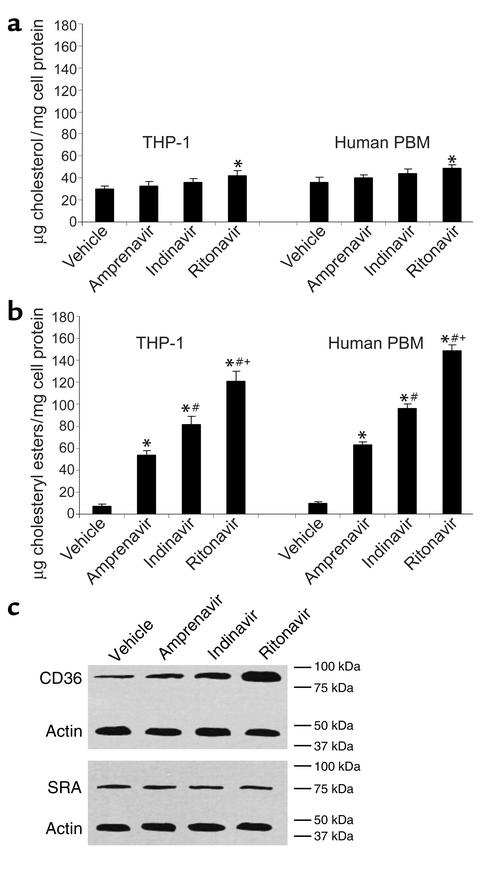
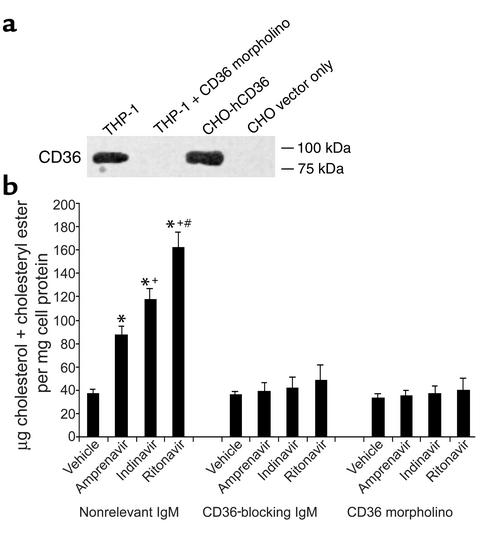
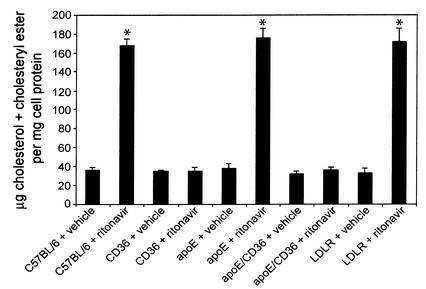
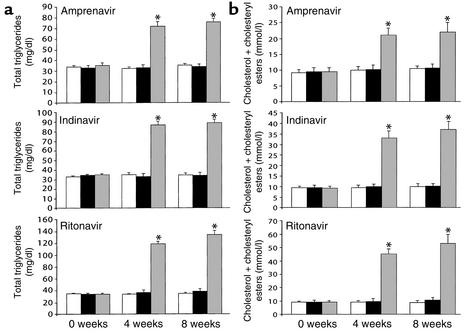
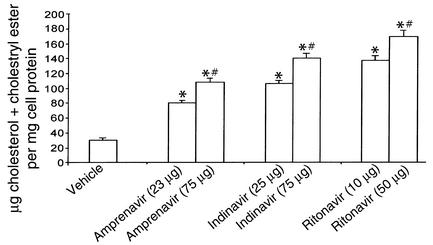
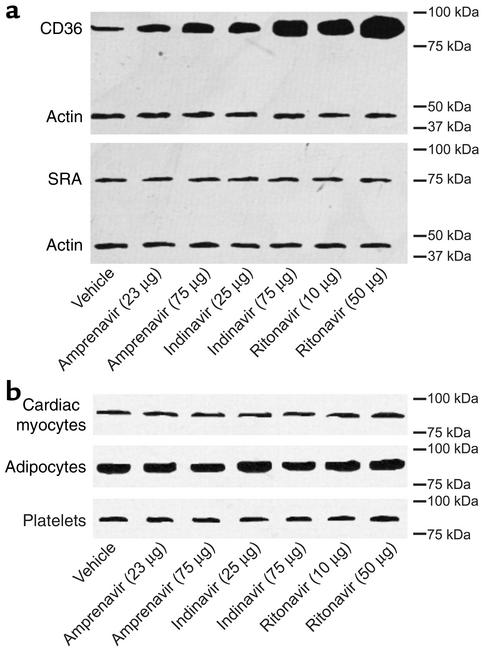
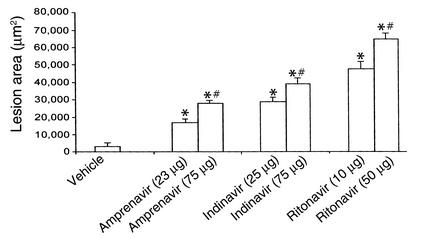
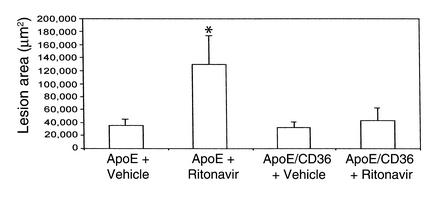
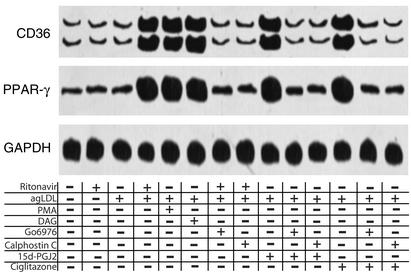
Protease inhibitors decrease the viral load in HIV patients, however the patients develop hypertriglyceridemia, hypercholesterolemia, and atherosclerosis. It has been assumed that protease inhibitor-dependent increases in atherosclerosis are secondary to the dyslipidemia. Incubation of THP-1 cells or human PBMCs with protease inhibitors caused upregulation of CD36 and the accumulation of cholesteryl esters. The use of CD36-blocking antibodies, a CD36 morpholino, and monocytes isolated from CD36 null mice demonstrated that protease inhibitor-induced increases in cholesteryl esters were dependent on CD36 upregulation. These data led to the hypothesis that protease inhibitors induce foam cell formation and consequently atherosclerosis by upregulating CD36 and cholesteryl ester accumulation independent of dyslipidemia. Studies with LDL receptor null mice demonstrated that low doses of protease inhibitors induce an increase in the level of CD36 and cholesteryl ester in peritoneal macrophages and the development of atherosclerosis without altering plasma lipids. Furthermore, the lack of CD36 protected the animals from protease inhibitor-induced atherosclerosis. Finally, ritonavir increased PPAR-gamma and CD36 mRNA levels in a PKC- and PPAR-gamma-dependent manner. We conclude that protease inhibitors contribute to the formation of atherosclerosis by promoting the upregulation of CD36 and the subsequent accumulation of sterol in macrophages.
Figures
Comment in
-
HIV protease inhibitors and atherosclerosis.J Clin Invest. 2003 Feb;111(3):317-8. doi: 10.1172/JCI17746. J Clin Invest. 2003. PMID: 12569155 Free PMC article. Review. No abstract available.
References
-
- Periard D, et al. Atherogenic dyslipidemia in HIV-infected individuals treated with protease inhibitors. The Swiss HIV Cohort Study. Circulation. 1999;100:700–705. - PubMed
-
- Riddle TM, Kuhel DG, Woollett LA, Fichtenbaum CJ, Hui DY. HIV protease inhibitor induces fatty acid and sterol biosynthesis in liver and adipose tissues due to the accumulation of activated sterol regulatory element-binding proteins in the nucleus. J. Biol. Chem. 2001;276:37514–37519. - PubMed
-
- Wensing AM, Reedijk M, Richter C, Boucher CA, Borleffs JC. Replacing ritonavir by nelfinavir or nelfinavir/saquinavir as part of highly active antiretroviral therapy leads to an improvement of triglyceride levels. AIDS. 2001;15:2191–2193. - PubMed
-
- Vergis EN, Paterson DL, Wagener MM, Swindells S, Singh N. Dyslipidaemia in HIV-infected patients: association with adherence to potent antiretroviral therapy. Int. J. STD AIDS. 2001;12:463–468. - PubMed
-
- Stein JH, et al. Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation. 2001;104:257–262. - PubMed
