

Case Reports
Giant infiltrating lipoma of the face: CT and MR imaging findings
Affiliations
- PMID: 12591650
- PMCID: PMC7974129
Item in Clipboard
Case Reports
Giant infiltrating lipoma of the face: CT and MR imaging findings
AJNR Am J Neuroradiol.
2003 Feb.
Abstract
Infiltrating lipoma is an uncommon mesenchymal neoplasm that characteristically infiltrates adjacent tissues and tends to recur after excision. This type of lipoma is extremely rare in the head and neck region. We report a case of a giant infiltrating lipoma of the face, studied with CT and MR imaging.
Figures
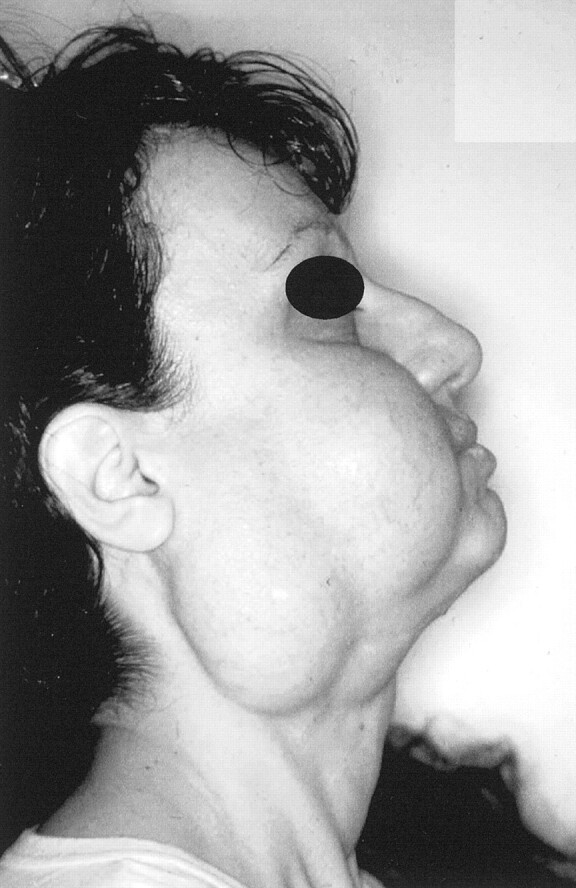
Photograph of a 37-year-old white female patient who presented with a 2-year history of slowly progressive swelling of the right cheek and parotidomasseteric and submandibular areas.
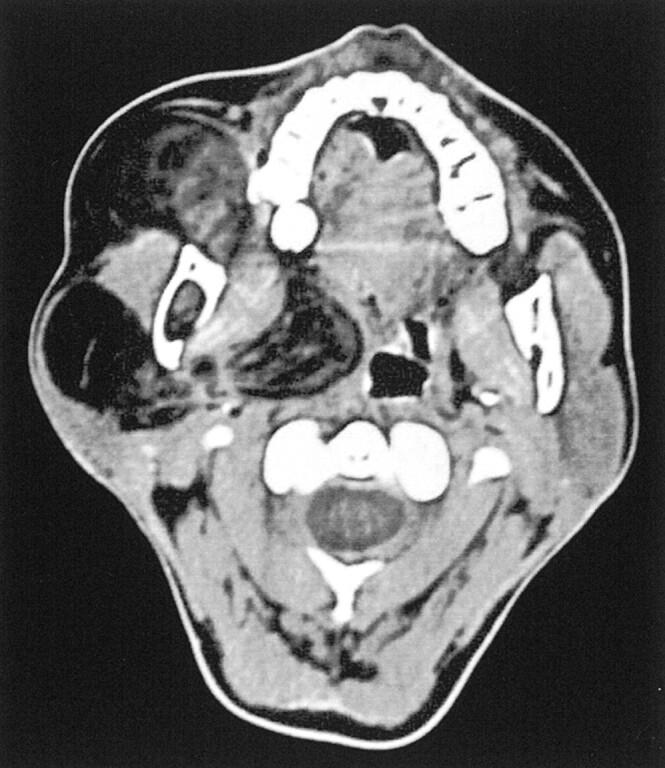
Axial contrast-enhanced CT scan shows an expansive, ill-defined, inhomogeneously hypoattenuated mass occupying the parotidomasseteric region and extending deeply toward the right parapharyngeal space. The parotid gland is compressed and displaced posteriorly. No contrast enhancement is evident. Linear densities within the lipomatous region are consistent with fibrous materials revealed by histologic examination.
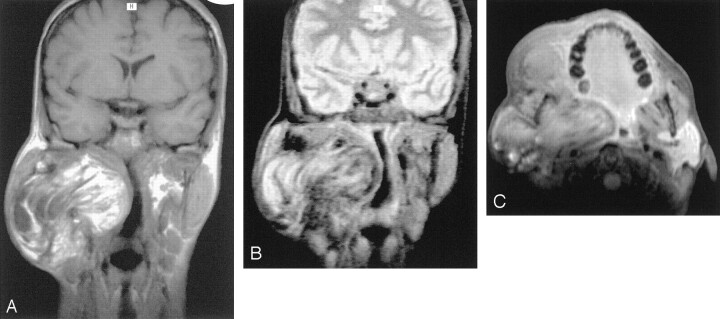
MR images obtained with a 1.0-T superconductive imaging unit. A, Coronal spin-echo T1-weighted MR image (512/17) shows an inhomogeneous hyperintense lesion located in the parotidomasseteric region and extending deeply toward the parapharyngeal space. B, On spin-echo T2-weighted MR image without fat suppression (2300/80), decreasing signal intensity is appreciable and irregular linear regions of markedly hypointense signal are present. C, Axial contrast-enhanced fat-suppressed spin-echo T1-weighted MR image (900/22) shows partial suppression of the lesion, consistent with fat. The lesion nevertheless shows ill-defined margins without a clear plane of cleavage between the mass and the adjacent muscular structures, especially the pterygoid and masseter muscles that appeared displaced and compressed. No evidence of contrast enhancement within the mass can be seen.

Photograph of surgical specimen. Removal of the mass was difficult, because the posterior part of the lesion was firmly attached to the surrounding muscles and the ramus of mandible. The gross appearance of the mass is that of an irregular, lobulated, firm fatty lesion with no evidence of encapsulation.
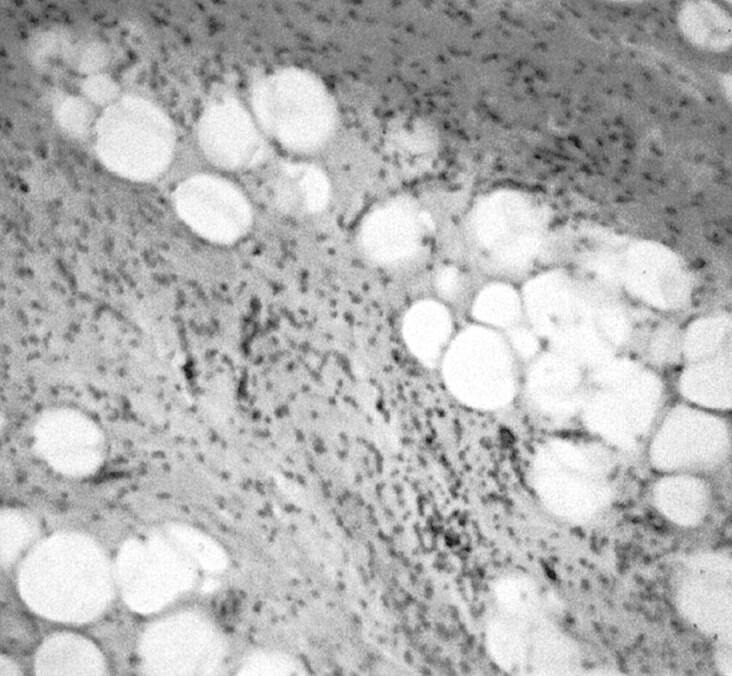
Pathologic specimen (hematoxylin and eosin; original magnification, ×400). The lesion is composed of uniform-appearing mature adipocytes, with the presence of myxoid hypocellular areas and infiltrates of inflammatory cells, especially lymphocytes. Diffuse infiltration of entrapped striated muscles can be seen; no evidence of lipoblasts, cellular atypism, or mitoses indicating liposarcoma is seen.
Similar articles
-
[Provocable tumor of the cheek as a manifestation of so-called "infiltrating lipoma" of the masseter muscle].Laryngorhinootologie. 1992 Jun;71(6):328-31. doi: 10.1055/s-2007-997306. Laryngorhinootologie. 1992. PMID: 1637456 German.
-
Infiltrating lipoma of the face.Ann Plast Surg. 1995 Sep;35(3):307-9. doi: 10.1097/00000637-199509000-00015. Ann Plast Surg. 1995. PMID: 7503527
-
[Lipoma of the forehead].Hautarzt. 2000 Sep;51(9):661-5. doi: 10.1007/s001050051191. Hautarzt. 2000. PMID: 11057392 German.
-
An infantile case of infiltrating lipoma in the buttock.J Pediatr Surg. 1991 Feb;26(2):230-2. doi: 10.1016/0022-3468(91)90921-f. J Pediatr Surg. 1991. PMID: 2023095 Review.
-
Infiltrating angiolipoma of the M. temporalis.Auris Nasus Larynx. 2000 Jul;27(3):265-9. doi: 10.1016/s0385-8146(99)00075-9. Auris Nasus Larynx. 2000. PMID: 10808117 Review.
Cited by
-
Case Report: Congenital infiltrating lipomatosis of face.Indian J Radiol Imaging. 2008 Nov;18(4):306-9. doi: 10.4103/0971-3026.43847. Indian J Radiol Imaging. 2008. PMID: 19774187 Free PMC article.
-
Excision of Bilobed Supraglottic Lipoma via Transoral Robotic Surgery.Indian J Otolaryngol Head Neck Surg. 2025 Jul;77(7):2629-2632. doi: 10.1007/s12070-025-05519-z. Epub 2025 May 21. Indian J Otolaryngol Head Neck Surg. 2025. PMID: 40503134
-
Unravelling the unique case of congenital infiltrating lipomatosis of face with its rare associations-A case report.J Oral Biol Craniofac Res. 2024 Nov-Dec;14(6):767-772. doi: 10.1016/j.jobcr.2024.10.006. Epub 2024 Oct 20. J Oral Biol Craniofac Res. 2024. PMID: 39497910 Free PMC article.
-
Large lipoma in the subglottic larynx: a case report.J Int Med Res. 2020 Jun;48(6):300060520928786. doi: 10.1177/0300060520928786. J Int Med Res. 2020. PMID: 32495672 Free PMC article.
-
Common and uncommon lesions of the vulva and vagina on magnetic resonance imaging: correlations with pathological findings.BJR Open. 2023 Jun 28;5(1):20230002. doi: 10.1259/bjro.20230002. eCollection 2023. BJR Open. 2023. PMID: 37389007 Free PMC article. Review.
References
-
- Kransdorf MJ. Benign soft-tissue tumors in a large referral population: distribution of specific diagnoses by age, sex, and location. AJR Am J Roentgenol 1995;164:395–402 - PubMed
-
- Piattelli A, Fioroni M, Rubini C. Intramuscular lipoma of the cheek: a case report. J Oral Maxillofac Surg 2000;58:817–819 - PubMed
-
- Lacey MS, Craig I. Infiltrating lipoma of the face. Ann Plast Surg 1995;35:307–309 - PubMed
-
- Pelissier A, Sawaf MH, Shabana AM. Infiltrating (intramuscular) benign lipoma of the head and neck. J Oral Maxillofac Surg 1991;49:1231–1236 - PubMed
-
- Bennhoff DF, Wood JW. Infiltrating lipomata of the head and neck. Laryngoscope 1978;88:839–848 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical