

Relation between heart rate, heart rhythm, and reverse left ventricular remodelling in response to carvedilol in patients with chronic heart failure: a single centre, observational study
- PMID: 12591834
- PMCID: PMC1767578
- DOI: 10.1136/heart.89.3.293
Relation between heart rate, heart rhythm, and reverse left ventricular remodelling in response to carvedilol in patients with chronic heart failure: a single centre, observational study
Abstract
Objective: To determine whether the process of reverse left ventricular remodelling in response to carvedilol is dependent on baseline heart rate (BHR), heart rhythm, or heart rate reduction (HRR) in response to carvedilol.
Design: Retrospective analysis of serial echocardiograms in 257 patients with chronic systolic heart failure at baseline and at 12-18 months after starting carvedilol. Reverse left ventricular remodelling was determined by changes in left ventricular end diastolic dimension (LVEDD), end systolic dimension (LVESD), and fractional shortening (LVFS).
Setting: Heart failure clinic within a university teaching hospital.
Main outcome measures: Changes in LVEDD, LVESD, and LVFS.
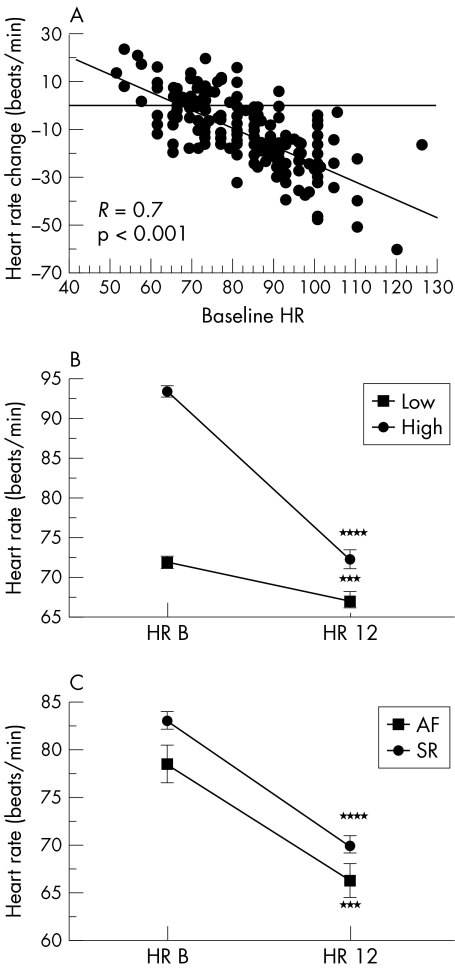
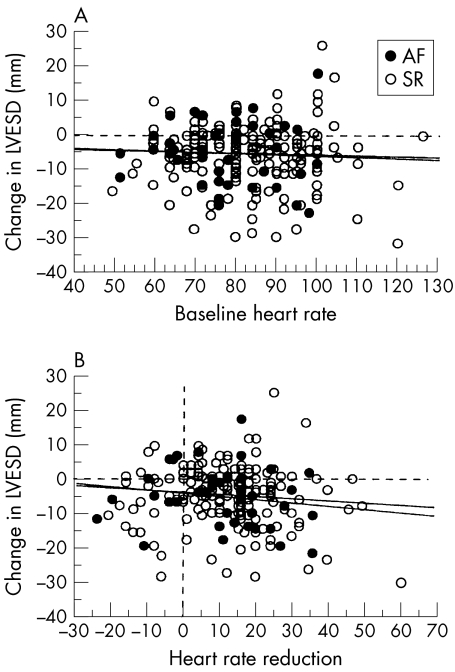
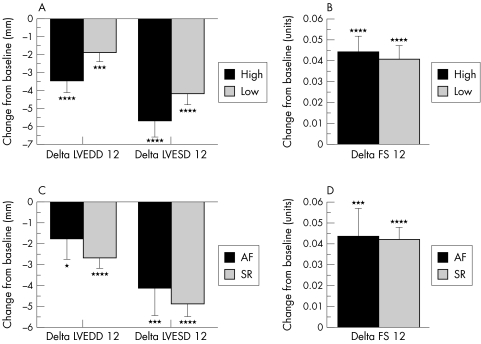
Results: LVEDD and LVESD decreased by 2.6 (0.4) mm and 4.9 (0.5) mm, respectively (mean (SEM)), and LVFS increased by 4.3 (0.5)% (all p < 0.0001 v baseline). Simple regression revealed no significant relation between BHR or HRR and the changes in LVEDD, LVESD, or LVFS. Stratification of patients into high and low BHR groups (above and below the mean) or according to the baseline heart rhythm (sinus rhythm v atrial fibrillation) showed no differences between groups in the extent of reverse left ventricular remodelling. Improvements in left ventricular function and dimensions were associated with significant improvements in New York Heart Association functional class.
Conclusions: The benefits of carvedilol in terms of reverse left ventricular remodelling and symptomatic improvement in patients with chronic heart failure are independent of BHR, heart rhythm, and the HRR that occurs in response to carvedilol.
Figures
Similar articles
-
Effects of carvedilol on left ventricular remodelling in chronic stable heart failure: a cardiovascular magnetic resonance study.Heart. 2004 Jul;90(7):760-4. doi: 10.1136/hrt.2003.015552. Heart. 2004. PMID: 15201244 Free PMC article. Clinical Trial.
-
Impact of concurrent amiodarone treatment on the tolerability and efficacy of carvedilol in patients with chronic heart failure.Heart. 1999 Nov;82(5):589-93. doi: 10.1136/hrt.82.5.589. Heart. 1999. PMID: 10525515 Free PMC article.
-
Beta-blockade therapy in chronic heart failure: diastolic function and mitral regurgitation improvement by carvedilol.Am Heart J. 2000 Apr;139(4):596-608. doi: 10.1016/s0002-8703(00)90036-x. Am Heart J. 2000. PMID: 10740140 Clinical Trial.
-
Left ventricular remodelling and improved long-term outcomes in chronic heart failure.Eur Heart J. 1998 Feb;19 Suppl B:B36-9. Eur Heart J. 1998. PMID: 9519350 Review.
-
Carvedilol: use in chronic heart failure.Expert Rev Cardiovasc Ther. 2007 Jan;5(1):21-31. doi: 10.1586/14779072.5.1.21. Expert Rev Cardiovasc Ther. 2007. PMID: 17187454 Review.
Cited by
-
Rate adaptive pacing in people with chronic heart failure increases peak heart rate but not peak exercise capacity: a systematic review.Heart Fail Rev. 2023 Jan;28(1):21-34. doi: 10.1007/s10741-022-10217-x. Epub 2022 Feb 9. Heart Fail Rev. 2023. PMID: 35138522 Free PMC article.
-
β-Blocker Doses and Heart Rate in Patients with Heart Failure: Results from the National Norwegian Heart Failure Registry.Biomed Hub. 2020 Feb 21;5(1):9-18. doi: 10.1159/000505474. eCollection 2020 Jan-Apr. Biomed Hub. 2020. PMID: 32775329 Free PMC article.
-
Chronic heart failure, chronotropic incompetence, and the effects of beta blockade.Heart. 2006 Apr;92(4):481-6. doi: 10.1136/hrt.2004.058073. Epub 2005 Sep 13. Heart. 2006. PMID: 16159968 Free PMC article.
-
A gender-based analysis of high school athletes using computerized electrocardiogram measurements.PLoS One. 2013;8(1):e53365. doi: 10.1371/journal.pone.0053365. Epub 2013 Jan 2. PLoS One. 2013. PMID: 23301064 Free PMC article.
-
Effects of β-adrenergic blockade on left ventricular remodeling among Hispanics and African Americans with chronic heart failure.Clin Cardiol. 2013 Oct;36(10):595-602. doi: 10.1002/clc.22164. Epub 2013 Jul 24. Clin Cardiol. 2013. PMID: 23893765 Free PMC article.
References
-
- DiLenarda A, Gregori D, Sinagra G, et al. Metoprolol in dilated cardiomyopathy: is it possible to identify factors predictive of improvement? The heart muscle disease study group. J Card Fail 1996;2:87–102. - PubMed
-
- Schleman KA, Lindenfeld JA, Lowes BD, et al. Predicting response to carvedilol for the treatment of heart failure: a multivariate retrospective analysis. J Card Fail 2001;7:4–12. - PubMed
-
- Metra M, Nardi M, Giubbini R, et al. Effects of short- and long-term carvedilol administration on rest and exercise hemodynamic variables, exercise capacity and clinical conditions in patients with idiopathic dilated cardiomyopathy. J Am Coll Cardiol 1994;24:1678–87. - PubMed
-
- Eichhorn EJ, Heesch CM, Risser RC, et al. Predictors of systolic and diastolic improvement in patients with dilated cardiomyopathy treated with metoprolol. J Am Coll Cardiol 1995;25:154–62. - PubMed
-
- Lechat P, Escolano S, Golmard JL, et al. Prognostic value of bisoprolol-induced hemodynamic effects in heart failure during the cardiac insufficiency bisoprolol study (CIBIS). Circulation 1997;96:2197–205. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical