

Neoadjuvant chemotherapy for extensive unilateral retinoblastoma
- PMID: 12598448
- PMCID: PMC1771557
- DOI: 10.1136/bjo.87.3.327
Neoadjuvant chemotherapy for extensive unilateral retinoblastoma
Abstract
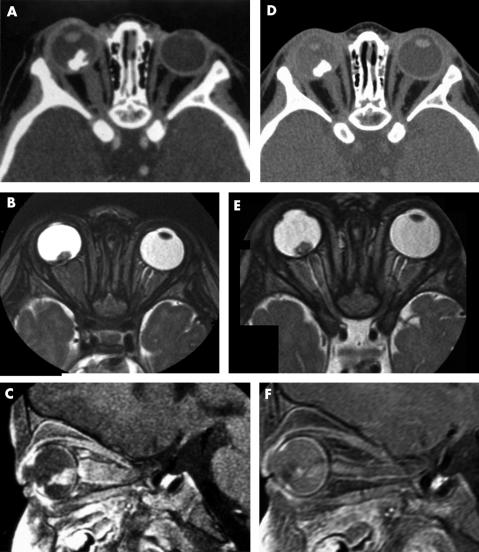
Aim: The role of neoadjuvant chemotherapy was studied when first line enucleation cannot be safely performed in unilateral extensive retinoblastoma (major buphthalmia or radiologically detectable optic nerve involvement).
Methods: Six patients, referred for unilateral retinoblastoma, presented with major buphthalmia (two) or optic nerve invasion (four): they were treated by neoadjuvant chemotherapy using etoposide and carboplatin.
Results: Good tumour response was observed in the two patients with buphthalmia and in three of four cases with optic nerve involvement. Meningeal progressive disease was observed in the last patient. The five patients without disease progression were then operated on: anterior enucleation in the patients with buphthalmia and enucleation via a double neurosurgical and ophthalmological approach with prechiasmatic optic nerve section in the other three cases. Postoperative chemotherapy was performed in these five patients. Local radiotherapy to the chiasmatic region and posterior part of the optic canal was necessary in only one patient. The non-operated patient died with disease progression 6 months after the diagnosis. The other five patients are alive with a follow up of 12, 15, 21, 36, and 40 months after stopping treatment.
Conclusion: Neoadjuvant chemotherapy can be useful in extensive unilateral retinoblastoma with buphthalmia and/or radiological optic nerve invasion at diagnosis.
Figures
References
-
- Shields JA, Shields CL, Suvarnamani C, et al. Retinoblastoma manifesting as orbital cellulitis. Am J Ophthalmol 1991;112:442–9. - PubMed
-
- Doz F, Neuenschwander S, Plantaz D, et al. Etoposide and carboplatin in extraocular retinoblastoma: a study by the Société Française d’Oncologie Pédiatrique. J Clin Oncol 1995;13:902–9. - PubMed
-
- Greenwald MJ, Strauss LC. Treatment of intraocular retinoblastoma with carboplatin and etoposide chemotherapy. Ophthalmology 1996;103:1989–97. - PubMed
-
- Kingston J, Hungerford JL, Madreperla SA et al. Results of combined chemotherapy and radiotherapy for advanced intraocular retinoblastoma. Arch Ophthalmol 1996;114:1339–43. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources