

Pilot investigation of hypothermia in neonates receiving extracorporeal membrane oxygenation
- PMID: 12598502
- PMCID: PMC1721509
- DOI: 10.1136/fn.88.2.f128
Pilot investigation of hypothermia in neonates receiving extracorporeal membrane oxygenation
Abstract
Background: Infants requiring extracorporeal membrane oxygenation (ECMO) support represent a high risk group in terms of cerebral injury. Mild hypothermia both during and after cerebral hypoxic ischaemia appears to be a promising strategy for offering neuroprotection.
Objective: To investigate whether mild hypothermia was both feasible and safe in infants receiving ECMO as a prelude to any formal assessment of this approach in a randomised trial.
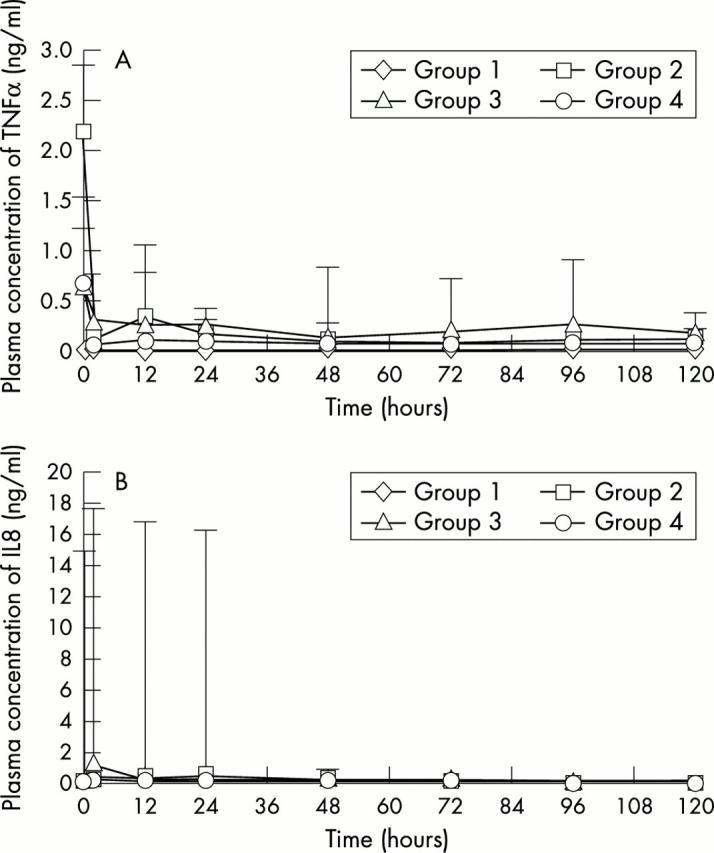
Methods: Twenty infants (body weight less than 5 kg) with severe cardiopulmonary insufficiency, referred for ECMO support at Glenfield Hospital, Leicester, were enrolled in this study. Twenty consecutive infants (compromising four groups of five) were studied. Baseline data were obtained from a control group who were run throughout their course at 37 degrees C. The patients in the next group were managed with a core temperature of 36 degrees C for the first 12 hours of their ECMO run, before being warmed up to 37 degrees C. After successful completion, the next group of five were cared for at 35 degrees C for the first 12 hours, and, there having been no previous complications, the final group were cared for at 34 degrees C for the first 12 hours. Patients were assessed clinically and biologically. In addition to routine laboratory tests, cytokines (interleukin 6, interleukin 8, tumour necrosis factor alpha, and C reactive protein) were measured and coagulation tests (D-dimer, thrombin-antithrombin III complex, plasmin-alpha(2)-antiplasmin complex) were performed serially for five days.
Results: There were no significant differences among the four groups in gestational age, birth weight, age at the time of ECMO, Apgar scores at one and five minutes, pH before cannulation, oxygenation index, duration of ECMO, and survival rate to discharge from hospital. No adverse effects of mild hypothermia were found on patient management during ECMO. Laboratory data for up to five days of ECMO also showed no difference among the four groups.
Conclusion: Mild hypothermia (34 degrees C) for the initial 12 hours of an ECMO run is feasible.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials