

Clinical concentrations of thioridazine kill intracellular multidrug-resistant Mycobacterium tuberculosis
- PMID: 12604522
- PMCID: PMC149316
- DOI: 10.1128/AAC.47.3.917-922.2003
Clinical concentrations of thioridazine kill intracellular multidrug-resistant Mycobacterium tuberculosis
Abstract
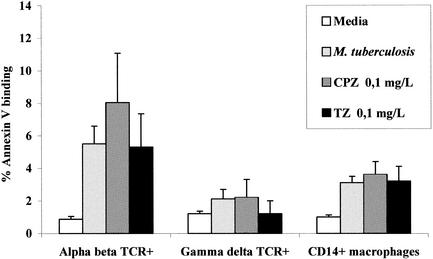
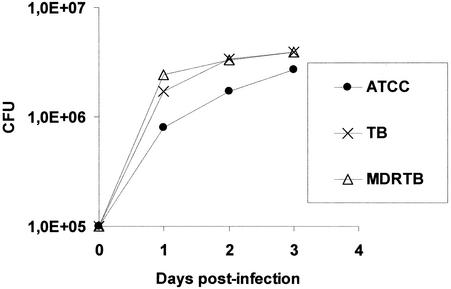
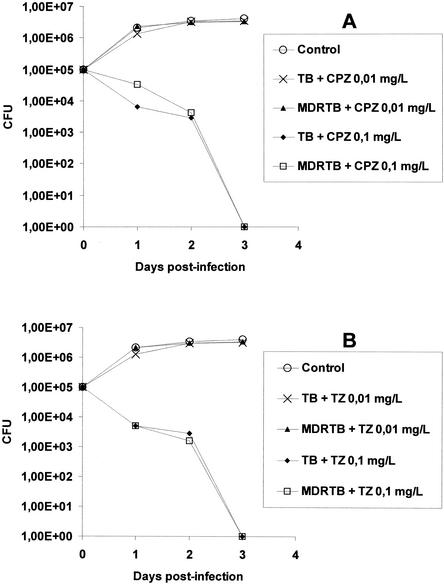
The phenothiazines chlorpromazine (CPZ) and thioridazine (TZ) have equal in vitro activities against antibiotic-sensitive and -resistant Mycobacterium tuberculosis. These compounds have not been used as anti-M. tuberculosis agents because their in vitro activities take place at concentrations which are beyond those that are clinically achievable. In addition, chronic administration of CPZ produces frequent severe side effects. Because CPZ has been shown to enhance the killing of intracellular M. tuberculosis at concentrations in the medium that are clinically relevant, we have investigated whether TZ, a phenothiazine whose negative side effects are less frequent and serious than those associated with CPZ, kills M. tuberculosis organisms that have been phagocytosed by human macrophages, which have nominal killing activities against these bacteria. Both CPZ and TZ killed intracellular antibiotic-sensitive and -resistant M. tuberculosis organisms when they were used at concentrations in the medium well below those present in the plasma of patients treated with these agents. These concentrations in vitro were not toxic to the macrophage, nor did they affect in vitro cellular immune processes. TZ thus appears to be a serious candidate for the management of a freshly diagnosed infection of pulmonary tuberculosis or as an adjunct to conventional antituberculosis therapy if the patient originates from an area known to have a high prevalence of multidrug-resistant M. tuberculosis isolates. Nevertheless, we must await the outcomes of clinical trials to determine whether TZ itself may be safely and effectively used as an antituberculosis agent.
Figures
Similar articles
-
Clinical concentrations of thioridazine enhance the killing of intracellular methicillin-resistant Staphylococcus aureus: an in vivo, ex vivo and electron microscopy study.In Vivo. 2004 Nov-Dec;18(6):787-94. In Vivo. 2004. PMID: 15646821
-
Activity of phenothiazines against antibiotic-resistant Mycobacterium tuberculosis: a review supporting further studies that may elucidate the potential use of thioridazine as anti-tuberculosis therapy.J Antimicrob Chemother. 2001 May;47(5):505-11. doi: 10.1093/jac/47.5.505. J Antimicrob Chemother. 2001. PMID: 11328759 Review.
-
In vitro and ex vivo activity of thioridazine derivatives against Mycobacterium tuberculosis.Int J Antimicrob Agents. 2007 Mar;29(3):338-40. doi: 10.1016/j.ijantimicag.2006.10.013. Epub 2007 Jan 18. Int J Antimicrob Agents. 2007. PMID: 17239569
-
Inhibition of the respiration of multi-drug resistant clinical isolates of Mycobacterium tuberculosis by thioridazine: potential use for initial therapy of freshly diagnosed tuberculosis.J Antimicrob Chemother. 1996 Dec;38(6):1049-53. doi: 10.1093/jac/38.6.1049. J Antimicrob Chemother. 1996. PMID: 9023652
-
The broad-spectrum antimycobacterial activities of phenothiazines, InVitro: somewhere in all of this there may be patentable potentials.Recent Pat Antiinfect Drug Discov. 2011 May;6(2):104-9. doi: 10.2174/157489111796064623. Recent Pat Antiinfect Drug Discov. 2011. PMID: 21517740 Review.
Cited by
-
Differential antibiotic susceptibilities of starved Mycobacterium tuberculosis isolates.Antimicrob Agents Chemother. 2005 Nov;49(11):4778-80. doi: 10.1128/AAC.49.11.4778-4780.2005. Antimicrob Agents Chemother. 2005. PMID: 16251329 Free PMC article.
-
Efflux pumps of Gram-negative bacteria: what they do, how they do it, with what and how to deal with them.Front Pharmacol. 2014 Jan 3;4:168. doi: 10.3389/fphar.2013.00168. eCollection 2014. Front Pharmacol. 2014. PMID: 24427138 Free PMC article.
-
Thioridazine inhibits gene expression control of the cell wall signaling pathway (CWI) in the human pathogenic fungus Paracoccidioides brasiliensis.Mol Genet Genomics. 2016 Jun;291(3):1347-62. doi: 10.1007/s00438-016-1184-1. Epub 2016 Mar 8. Mol Genet Genomics. 2016. PMID: 26956010
-
Energy metabolism and drug efflux in Mycobacterium tuberculosis.Antimicrob Agents Chemother. 2014 May;58(5):2491-503. doi: 10.1128/AAC.02293-13. Epub 2014 Mar 10. Antimicrob Agents Chemother. 2014. PMID: 24614376 Free PMC article. Review.
-
Reduced emergence of isoniazid resistance with concurrent use of thioridazine against acute murine tuberculosis.Antimicrob Agents Chemother. 2014 Jul;58(7):4048-53. doi: 10.1128/AAC.02981-14. Epub 2014 May 5. Antimicrob Agents Chemother. 2014. PMID: 24798290 Free PMC article.
References
-
- Amaral, L., and J. E. Kristiansen. 2000. Phenothiazines: an alternative to conventional therapy for the initial management of suspected multi-drug resistant tuberculosis. Int. J. Antimicrob. Agents 14:173-176. - PubMed
-
- Amaral, L., and J. E. Kristiansen. 2001. Phenothiazines: potential management of Creutzfeldt-Jacob disease and its variants. Int. J. Antimicrob. Agents 18:411-417. - PubMed
-
- Amaral, L., J. E. Kristiansen, and V. Lorian. 1990. Synergistic effect of chlorpromazine on the activity of some antibiotics. J. Antimicrob. Chemother. 30:556-558. - PubMed
-
- Amaral, L., J. E. Kristiansen, L. S. Abebe, and W. Millet. 1996. Inhibition of the respiration of multi-drug resistant clinical isolates of Mycobacterium tuberculosis by thioridazine: potential use for initial therapy of freshly diagnosed tuberculosis. J. Antimicrob. Chemother. 38:1049-1053. - PubMed
-
- Amaral, L., J. E. Kristiansen, M. Viveiros, and J. Atouguia. 2001. Activity of phenothiazines against antibiotic-resistant Mycobacterium tuberculosis: a review supporting further studies that may elucidate the potential use of thioridazine as an anti-tuberculosis therapy. J. Antimicrob. Chemother. 47:505-511. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
