

Laparoscopic total mesorectal excision: a consecutive series of 100 patients
- PMID: 12616116
- PMCID: PMC1514324
- DOI: 10.1097/01.SLA.0000055270.48242.D2
Laparoscopic total mesorectal excision: a consecutive series of 100 patients
Abstract
Objective: To analyze total mesorectal excision (TME) for rectal cancer by the laparoscopic approach during a prospective nonrandomized trial.
Summary background data: Improved local control and survival rates in the treatment of rectal cancer have been reported after TME.
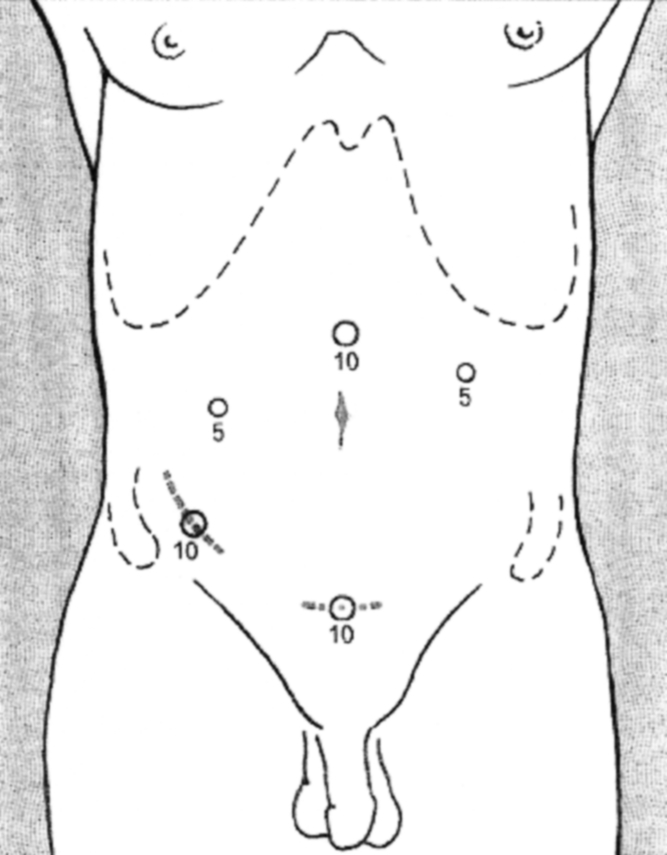
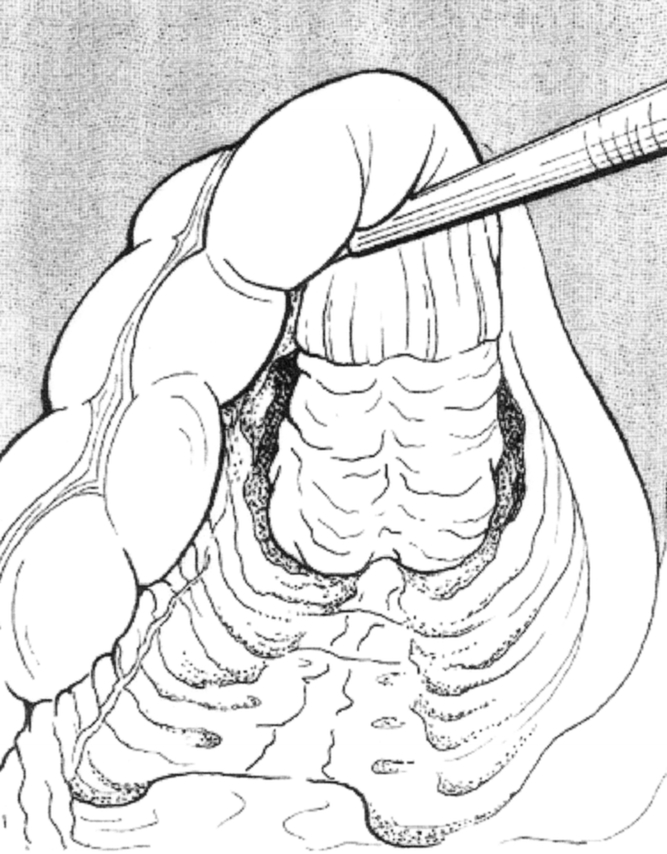
Methods: The authors conducted a prospective consecutive series of 100 laparoscopic TMEs for low and mid-rectal tumors. All patients had a sphincter-saving procedure. Case selection, surgical technique, and clinical and oncologic results were reviewed.
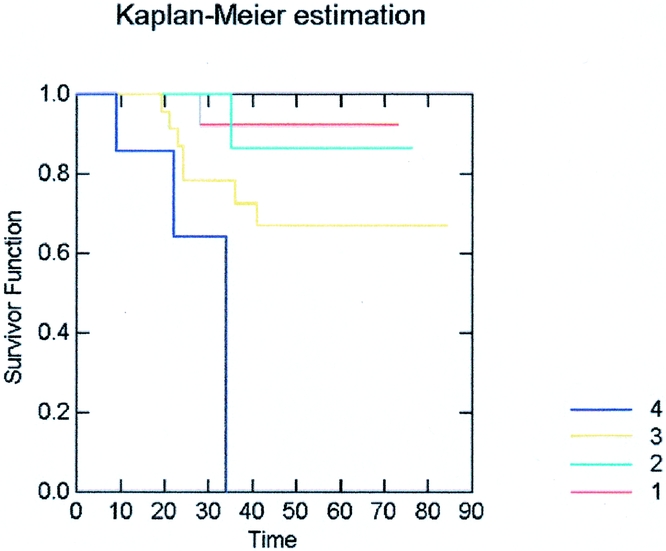
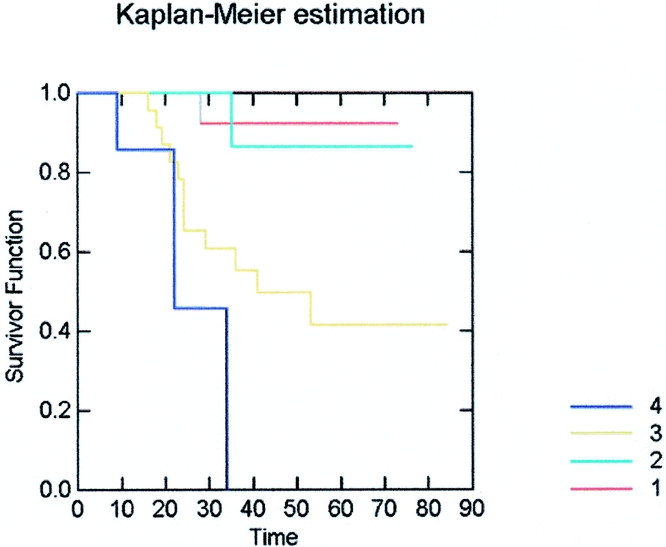
Results: The distal limit of rectal neoplasm was on average 6.1 (range 3-12) cm from the anal verge. The mean operative time was 250 (range 110-540) minutes. The conversion rate was 12%. Excluding the patient who stayed 104 days after a severe fistula and reoperation, the mean postoperative stay was 12.05 (range 5-53) days. The 30-day mortality was 2% and the overall postoperative morbidity was 36%, including 17 anastomotic leaks. Of 87 malignant cases, 70 (80.4%) had a minimum follow-up of 12 months, with a median follow-up of 45.7 (range 12-72) months. During this period 18.5% (13/70) died of cancer and 8.5% (6/70) are alive with metastatic disease. The port-site metastasis rate was 1.4% (1/70): a rectal cancer stage IV presented with a parietal recurrence at 17 months after surgery. The locoregional pelvic recurrence rate was 4.2% (3/70): three rectal cancers stage III at 19, 13, and 7 postoperative months.
Conclusions: Laparoscopic TME is a feasible but technically demanding procedure (12% conversion rate). This series confirms the safety of the procedure, while oncologic results are at present comparable to the open published series with the limitation of a short follow-up period. Further studies and possibly randomized series will be necessary to evaluate long-term clinical outcome in cancer patients.
Figures

References
-
- Heald RJ, Moran BJ, Ryall RDH, et al. The Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg. 1998; 133: 894–899. - PubMed
-
- Smedh K, Olsson L, Johansson H, et al. Reduction of postoperative morbidity and mortality in patients with rectal cancer following the introduction of a colorectal unit. Br J Surg. 2001; 88: 273–277. - PubMed
-
- Carlsen E, Schlichting E, Guldvog I, et al. Effect of the introduction of total mesorectal excision for the treatment of rectal cancer. Br J Surg. 1998; 85: 526–529. - PubMed
-
- Sobin LH, Wittekind CH. TNM classification of malignant tumours. 5th ed. Hoboken NJ: Wiley & Sons, Inc.; 1997.
-
- MacFarlane JK, Ryall RDH, Heald RJ. Mesorectal excision for rectal cancer. Lancet. 1993; 341: 457–460. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
