

Definitive surgical treatment of infected or exposed ventral hernia mesh
- PMID: 12616130
- PMCID: PMC1514321
- DOI: 10.1097/01.SLA.0000055278.80458.D0
Definitive surgical treatment of infected or exposed ventral hernia mesh
Abstract
Objective: To discuss the difficulties in dealing with infected or exposed ventral hernia mesh, and to illustrate one solution using an autogenous abdominal wall reconstruction technique.
Summary background data: The definitive treatment for any infected prosthetic material in the body is removal and substitution. When ventral hernia mesh becomes exposed or infected, its removal requires a solution to prevent a subsequent hernia or evisceration.
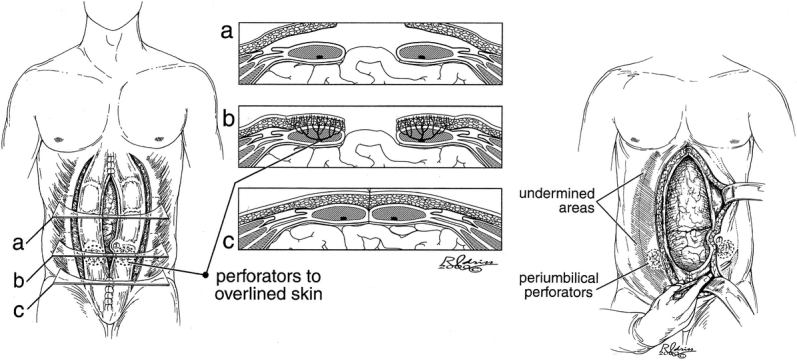
Methods: Eleven patients with ventral hernia mesh that was exposed, nonincorporated, with chronic drainage, or associated with a spontaneous enterocutaneous fistula were referred by their initial surgeons after failed local wound care for definitive management. The patients were treated with radical en bloc excision of mesh and scarred fascia followed by immediate abdominal wall reconstruction using bilateral sliding rectus abdominis myofascial advancement flaps.
Results: Four of the 11 patients treated for infected mesh additionally required a bowel resection. Transverse defect size ranged from 8 to 18 cm (average 13 cm). Average procedure duration was 3 hours without bowel repair and 5 hours with bowel repair. Postoperative length of stay was 5 to 7 days without bowel repair and 7 to 9 days with bowel repair. Complications included hernia recurrence in one case and stitch abscesses in two cases. Follow-up ranges from 6 to 54 months (average 24 months).
Conclusions: Removal of infected mesh and autogenous flap reconstruction is a safe, reliable, and one-step surgical solution to the problem of infected abdominal wall mesh.
Figures


References
-
- Luijendijk RW, Hop WCJ, van den Tol MP, et al. A comparison of suture repair with mesh repair for incisional hernia. N Engl J Med. 2000; 343: 392–397. - PubMed
-
- Leber GE, Garb JL, Alexander AI, et al. Long-term complications associated with prosthetic repair of incisional hernias. Arch Surg. 1998; 133: 378–382. - PubMed
-
- White TH, Santos MC, Thompson JS. Factors affecting wound complications associated with prosthetic repair of incisional hernias. Am Surg. 1998; 133: 378–382.
-
- Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990; 86: 519–525. - PubMed
-
- Saulis AS, Dumanian GA. Periumbilical rectus abdominis perforator preservation significantly reduces superficial wound complications in “separation of parts” hernia repairs. Plast Reconstr Surg. 2002; 109: 2275–2280. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
