

Number needed to treat (NNT): implication in rheumatology clinical practice
- PMID: 12634229
- PMCID: PMC1754501
- DOI: 10.1136/ard.62.4.316
Number needed to treat (NNT): implication in rheumatology clinical practice
Abstract
Objective: To calculate the number needed to treat (NNT) and number needed to harm (NNH) from the data in rheumatology clinical trials and systematic reviews.
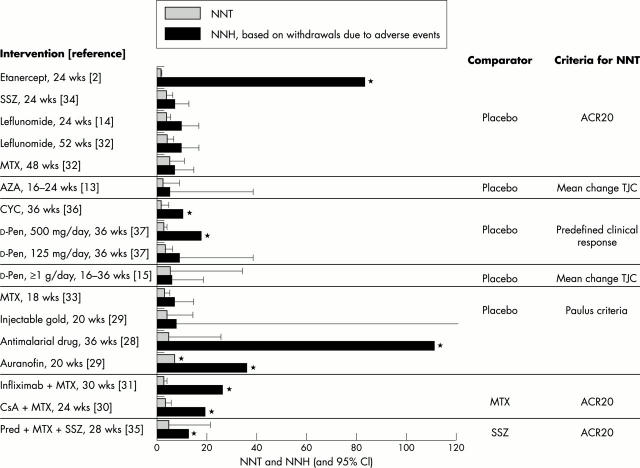
Methods: The NNTs for the clinically important outcome measures in the rheumatology systematic reviews from the Cochrane Library, issue 2, 2000 and in the original randomised, double blind, controlled trials were calculated. The measure used for calculating the NNT in rheumatoid arthritis (RA) interventions was the American College of Rheumatology 20% improvement or Paulus criteria; in osteoarthritis (OA) interventions, the improvement of pain; and in systemic sclerosis (SSc) interventions, the improvement of Raynaud's phenomenon. The NNH was calculated from the rate of withdrawals due to adverse events from the treatment.
Results: The data required for the calculation of the NNT were available in 15 systematic reviews and 11 original articles. For RA interventions, etanercept treatment for six months had the smallest NNT (1.6; 95% confidence interval (CI) 1.4 to 2.0), whereas leflunomide had the largest NNH (9.6; 95% CI 6.8 to 16.7). For OA treatment options, only etodolac and tenoxicam produced significant pain relief compared with placebo (NNT=4.4; 95% CI 2.4 to 24.4 and 3.8; 95% CI 2.5 to 7.3, respectively). For SSc interventions, none were shown to be efficacious in improving Raynaud's phenomenon because the 95% CI of the NNT was infinite.
Conclusions: The NNT and NNH are helpful for clinicians, enabling them to translate the results from clinical trials and systematic reviews to use in routine clinical practice. Both NNT and NNH should be accompanied by a limited 95% CI and adjusted for the individual subject's baseline risk.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
