

Treatment of patients with gastro-entero-pancreatic (GEP) tumours with the novel radiolabelled somatostatin analogue [177Lu-DOTA(0),Tyr3]octreotate
- PMID: 12634971
- PMCID: PMC1998890
- DOI: 10.1007/s00259-002-1050-8
Treatment of patients with gastro-entero-pancreatic (GEP) tumours with the novel radiolabelled somatostatin analogue [177Lu-DOTA(0),Tyr3]octreotate
Abstract
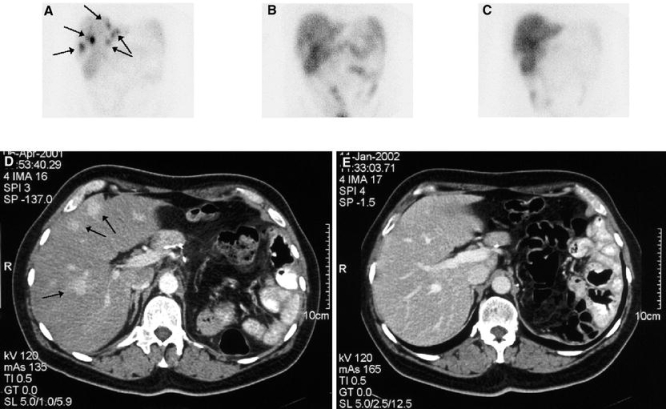
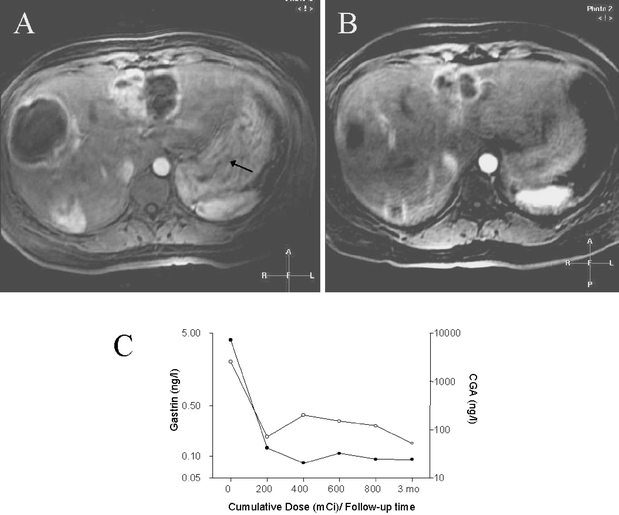
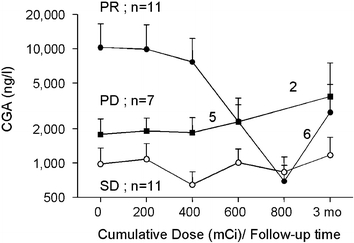
Medical treatment and chemotherapy are seldom successful in achieving objective tumour reduction in patients with metastatic neuroendocrine tumours. Treatment with the radiolabelled somatostatin analogue [(90)Y-DOTA(0),Tyr(3)]octreotide may result in partial remissions in 10-25% of patients. The newer analogue [DOTA(0),Tyr(3)]octreotate (octreotate) has a ninefold higher affinity for the somatostatin receptor subtype 2 as compared with [DOTA(0),Tyr(3)]octreotide. Also, labelled with the beta- and gamma-emitting radionuclide (177)Lu, it has proved very successful in achieving tumour regression in animal models. The effects of (177)Lu-octreotate therapy were studied in 35 patients with neuroendocrine gastro-entero-pancreatic (GEP) tumours who underwent follow-up for 3-6 months after receiving their final dose. Patients were treated with doses of 100, 150 or 200 mCi (177)Lu-octreotate, to a final cumulative dose of 600-800 mCi, with treatment intervals of 6-9 weeks. Nausea and vomiting within the first 24 h after administration were present in 30% and 14% of the administrations, respectively. WHO toxicity grade 3 anaemia, leucocytopenia and thrombocytopenia occurred after 0%, 1% and 1% of the administrations, respectively. Serum creatinine and creatinine clearance did not change significantly. The effects of the therapy on tumour size were evaluable in 34 patients. Three months after the final administration, complete remission was found in one patient (3%), partial remission in 12 (35%), stable disease in 14 (41%) and progressive disease in seven (21%), including three patients who died during the treatment period. Tumour response was positively correlated with a high uptake on the octreoscan, limited hepatic tumour mass and a high Karnofsky Performance Score. Because of the limited efficacy of alternative therapies, many physicians currently adopt an expectant attitude when dealing with patients with metastatic GEP tumours. However, in view of the high success rate of therapy with (177)Lu-octreotate and the absence of serious side-effects, we advocate its use in patients with GEP tumours without waiting for tumour progression.
Figures
References
-
- Arnold R, Benning R, Neuhaus C, Rolwage M, Trautmann ME. Gastroenteropancreatic endocrine tumours: effect of Sandostatin on tumour growth. The German Sandostatin Study Group. Digestion 1993; 54 (Suppl 1):72–75. - PubMed
-
- Janson ET, Oberg K. Long-term management of the carcinoid syndrome. Treatment with octreotide alone and in combination with alpha-interferon. Acta Oncol 1993; 32:225–229. - PubMed
-
- Ducreux M, Ruszniewski P, Chayvialle JA, Blumberg J, Cloarec D, Michel H, Raymond JM, Dupas JL, Gouerou H, Jian R, Genestin E, Hammel P, Rougier P. The antitumoral effect of the long-acting somatostatin analog lanreotide in neuroendocrine tumors. Am J Gastroenterol 2000; 95:3276–3281. - DOI - PubMed
-
- Valkema R, de Jong M, Bakker WH, Breeman WAP, Kooij PPM, Lugtenburg PJ, de Jong FH, Christiansen A, Kam BLR, de Herder WW, Stridsberg M, Lindemans J, Ensing G, Krenning EP. Phase I study of peptide receptor radionuclide therapy with [111In-DTPA0]octreotide: the Rotterdam experience. Semin Nucl Med 2002; 32:110–122. - PubMed
-
- McCarthy KE, Woltering EA, Espenan GD, Cronin M, Maloney TJ, Anthony LB. In situ radiotherapy with 111In-pentetreotide: initial observations and future directions. Cancer J Sci Am 1998; 4:94-102. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
