

Lumbar root compression in the lateral recess: MR imaging, conventional myelography, and CT myelography comparison with surgical confirmation
- PMID: 12637281
- PMCID: PMC7973614
Lumbar root compression in the lateral recess: MR imaging, conventional myelography, and CT myelography comparison with surgical confirmation
Abstract
Background and purpose: Previous authors have shown that conventional myelography is superior to plain CT in the assessment of root compression in the lateral recess, but this question has never been evaluated with respect to MR imaging of the lumbar level. Our purpose was to assess the accuracy of MR imaging, conventional myelography, and postmyelography CT (CT myelography) of the lumbar level in identifying degenerative lateral recess root compression with surgical confirmation.
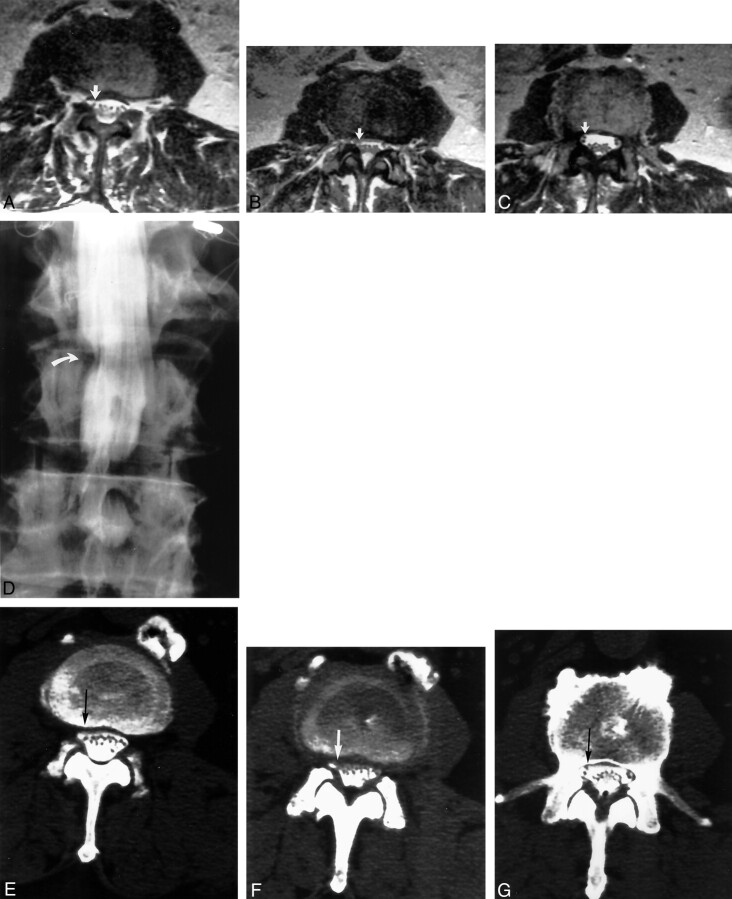
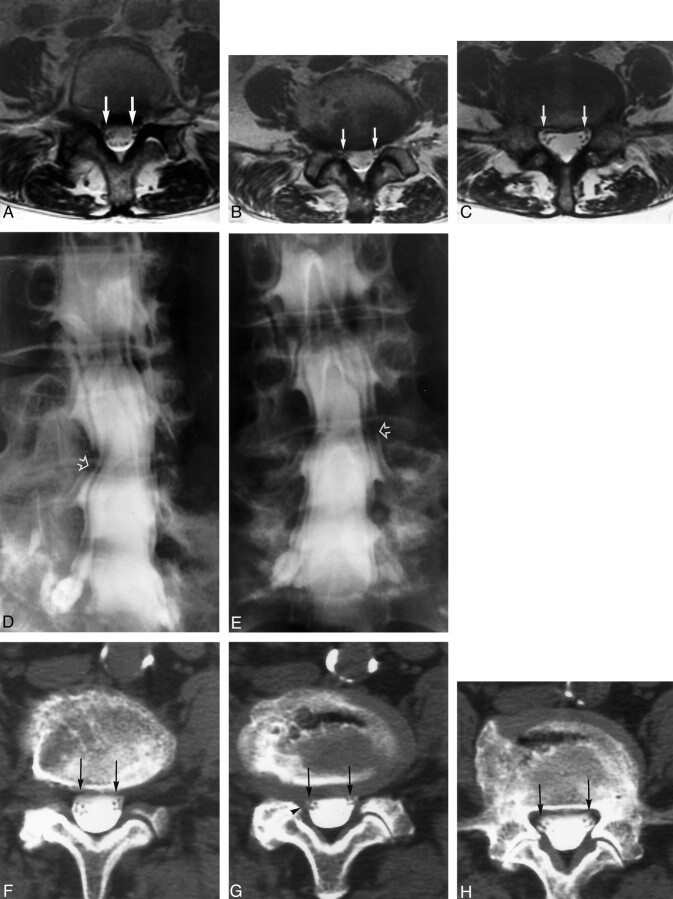
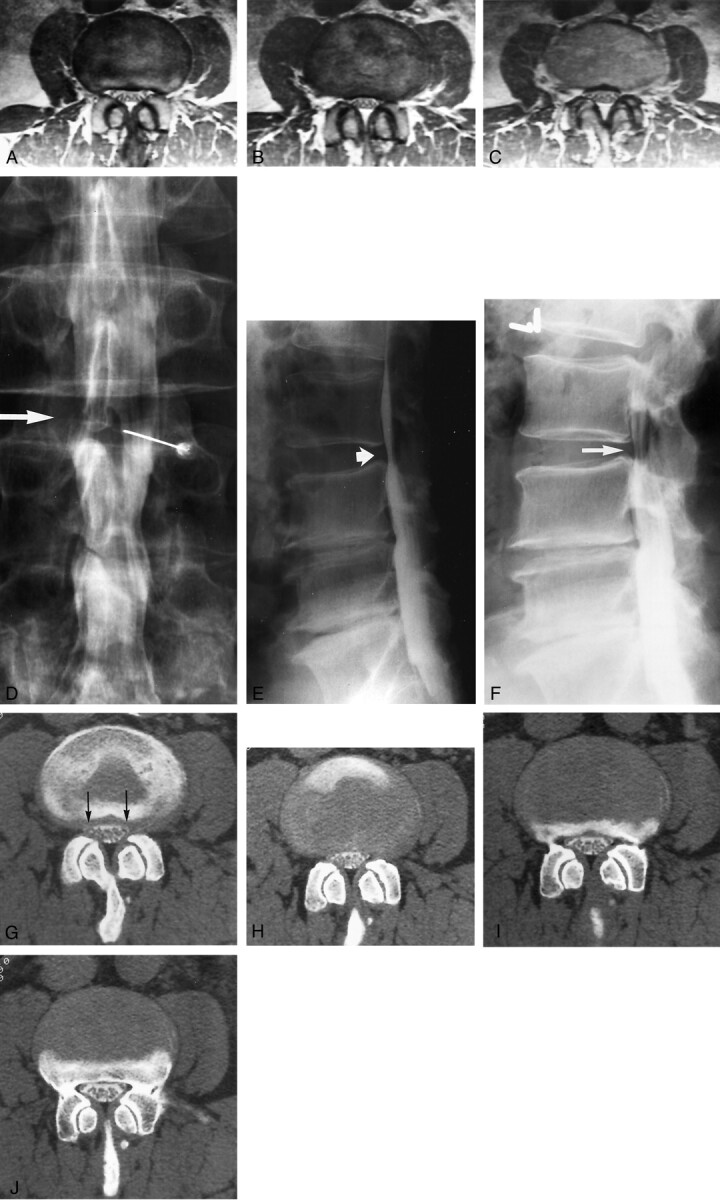
Methods: MR imaging, conventional myelography, and CT myelography of the lumbar level were assessed in the imaging of 58 lateral recesses at 38 lumbar levels in 26 patients who underwent surgery for radiculopathy with degenerative lateral recess abnormality. Each lateral recess was graded as normal, small without root compression, small with root compression, or severe root compression.
Results: MR imaging underestimated root compression in 28% to 29% of the cases in which root impingement was surgically confirmed. Conventional myelography underestimated root compression in only 5% to 7% of the cases and correctly predicted impingement in 93% to 95%. CT myelography underestimated root compression in 38% of the surgically confirmed cases.
Conclusion: MR imaging significantly underestimated root compression caused by degenerative changes in the lateral recess. Although MR imaging is a superb study when used in the search for degenerative disk disease and disk protrusion, conventional myelography is a crucial supplemental study that is necessary to confirm degenerative root impingement in the lateral recess as the cause of radiculopathy.
Figures
Comment in
-
Myelography: still the gold standard.AJNR Am J Neuroradiol. 2003 Mar;24(3):298. AJNR Am J Neuroradiol. 2003. PMID: 12637270 Free PMC article. No abstract available.
References
-
- McCarron RF, Wimpee MW, Hudkins PG, Laros GS. The inflammatory effect of nucleus pulposus: a possible element in the pathogenesis of low-back pain. Spine 1987;12:760–764 - PubMed
-
- Franson RC, Saal JS, Saal JA. Human disc phospholipase A2 is inflammatory. Spine 1992[suppl 6] 17:S129–S132 - PubMed
-
- Olmarker K, Rydevik B, Nordborg C. Autologous nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots. Spine 1993;18:1425–1432 - PubMed
-
- Saal JS. The role of inflammation in lumbar pain. Spine 1995;20:1821–1827 - PubMed
-
- Olmarker K, Blomquist J, Strömberg J, Nannmark U, Thomsen P, Rydevik B. Inflammatogenic properties of nucleus pulposus. Spine 1995;20:665–669 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical