

Five year results of viscocanalostomy
- PMID: 12642307
- PMCID: PMC1771626
- DOI: 10.1136/bjo.87.4.441
Five year results of viscocanalostomy
Abstract
Aim: To prospectively study the success rate and complications of viscocanalostomy, a non-penetrating glaucoma surgery.
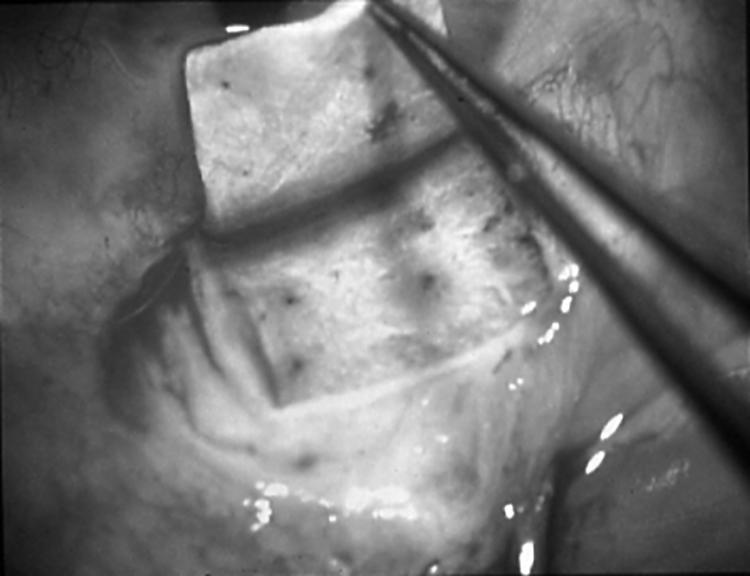
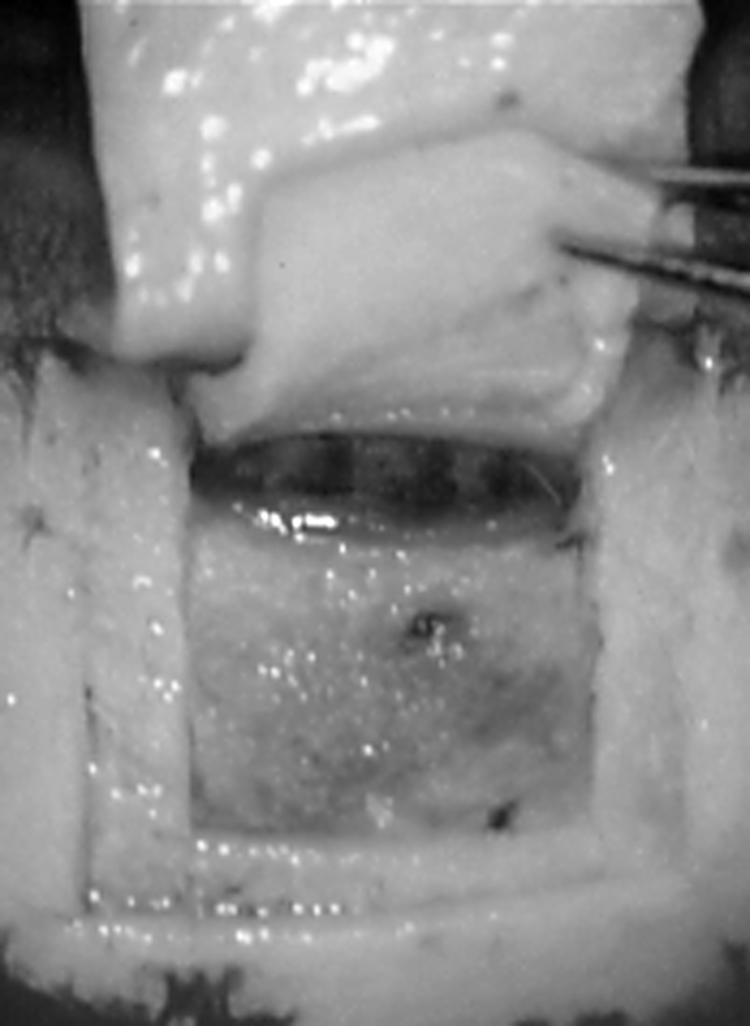
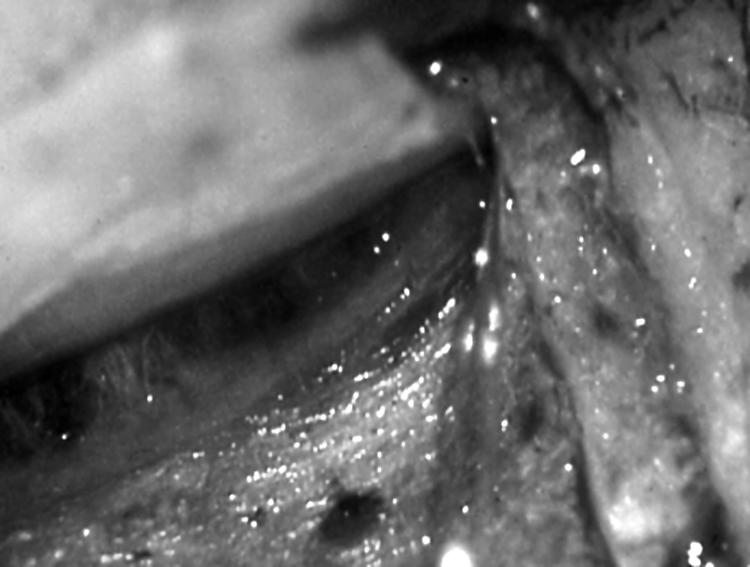
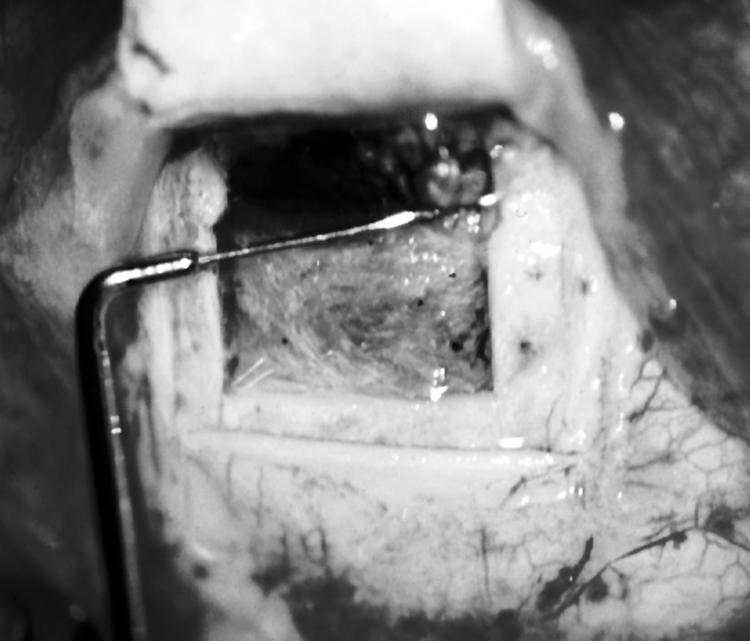
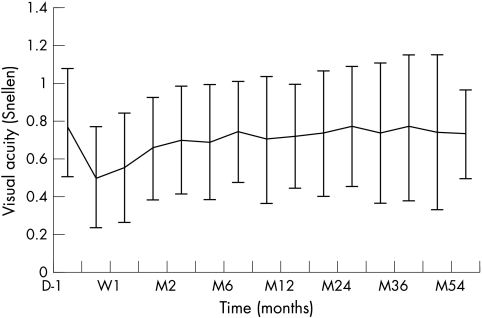
Methods: Prospective non-randomised consecutive case series of 57 eyes (57 patients) with medically uncontrolled primary and secondary open angle glaucoma. Viscocanalostomy was performed on all participants with injection of viscoelastic in the surgically created ostia of Schlemm's canal as well as in the scleral bed, the superficial scleral flap was loosely sutured. Intraocular pressure, visual acuity, and number of goniopunctures were measured.
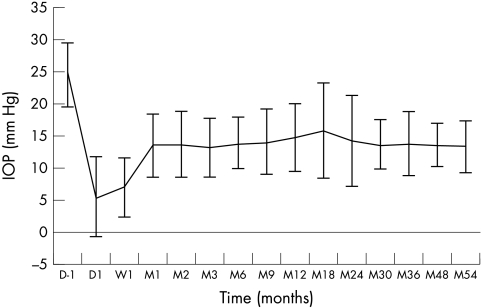
Results: The mean follow up period was 34.1 months. The mean preoperative intraocular pressure (IOP) was 24.6 mm Hg; while the mean postoperative IOP was 5.6 mm Hg at day 1 and 13.9 mm Hg at 36 month. Patients who achieved IOP below 21 mm Hg with or without medication were 90% at 60 months, complete success rate (IOP<21 mm Hg without medication) was 60% at 60 months. 21 patients (37%) needed Nd:YAG goniopuncture postoperatively to control raised IOP, mean time for goniopuncture application was 9.4 months, mean pre-goniopuncture IOP was 20.4 mm Hg and mean postgoniopuncture IOP was 12.6 mm Hg (p <0.0001).
Conclusion: Viscocanalostomy appears to be a promising modification of filtering surgery.
Figures
Similar articles
-
Modified viscocanalostomy in the Chinese population with open angle glaucoma: a 10-year follow-up results.Int J Ophthalmol. 2019 Mar 18;12(3):429-435. doi: 10.18240/ijo.2019.03.13. eCollection 2019. Int J Ophthalmol. 2019. PMID: 30918812 Free PMC article.
-
A New Expander for Schlemm Canal Surgery in Primary Open-angle Glaucoma-Interim Clinical Results.J Glaucoma. 2016 Aug;25(8):657-62. doi: 10.1097/IJG.0000000000000397. J Glaucoma. 2016. PMID: 26950578
-
Viscocanalostomy for primary open-angle glaucoma: the Gross Pankow experience.J Cataract Refract Surg. 2000 Sep;26(9):1367-73. doi: 10.1016/s0886-3350(00)00449-1. J Cataract Refract Surg. 2000. PMID: 11020622
-
[Non-penetrating filtering surgery: concept, technique and results].Arq Bras Oftalmol. 2006 Jul-Aug;69(4):605-13. doi: 10.1590/s0004-27492006000400029. Arq Bras Oftalmol. 2006. PMID: 17119741 Review. Portuguese.
-
[Non penetrating filtering surgery, evolution and results].J Fr Ophtalmol. 2002 May;25(5):527-36. J Fr Ophtalmol. 2002. PMID: 12048520 Review. French.
Cited by
-
Recent Advances in the Surgical Management of Glaucoma in Exfoliation Syndrome.J Glaucoma. 2018 Jul;27 Suppl 1(Suppl 1):S95-S101. doi: 10.1097/IJG.0000000000000918. J Glaucoma. 2018. PMID: 29965903 Free PMC article. Review.
-
Modified viscocanalostomy in the Chinese population with open angle glaucoma: a 10-year follow-up results.Int J Ophthalmol. 2019 Mar 18;12(3):429-435. doi: 10.18240/ijo.2019.03.13. eCollection 2019. Int J Ophthalmol. 2019. PMID: 30918812 Free PMC article.
-
Canaloplasty versus Viscocanalostomy in Primary Open Angle Glaucoma.Electron Physician. 2017 Jan 25;9(1):3665-3671. doi: 10.19082/3665. eCollection 2017 Jan. Electron Physician. 2017. PMID: 28243422 Free PMC article.
-
Management of exfoliative glaucoma: challenges and solutions.Clin Ophthalmol. 2015 May 22;9:907-19. doi: 10.2147/OPTH.S77570. eCollection 2015. Clin Ophthalmol. 2015. PMID: 26045655 Free PMC article. Review.
-
The efficacy of viscocanalostomy for uncontrollable primary open-angle glaucoma in a developing country.Indian J Ophthalmol. 2013 Feb;61(2):71-3. doi: 10.4103/0301-4738.107196. Indian J Ophthalmol. 2013. PMID: 23412524 Free PMC article.
References
-
- Watson PG, Jakeman C, Ozturk M, et al. The complications of trabeculectomy (a 20-year follow-up). Eye 1990;4:425–38. - PubMed
-
- Kao SF, Lichter PR, Musch DC. Anterior chamber depth following filtration surgery. Ophthalmic Surg 1989;20:332–6. - PubMed
-
- Stewart WC, Shields MB. Management of anterior chamber depth after trabeculectomy. Am J Ophthalmol 1988;106:41–4 - PubMed
-
- Brubaker RF, Pederson JE. Ciliochoroidal detachment. Surv Ophthalmol 1983;27:281–9. - PubMed
-
- Gressel MG, Parrish RK II, Heuer DK. Delayed nonexpulsive suprachoroidal hemorrhage. Arch Ophthalmol 1984;102:1757–60. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical