

Anti-cytokine autoantibodies in autoimmunity: preponderance of neutralizing autoantibodies against interferon-alpha, interferon-omega and interleukin-12 in patients with thymoma and/or myasthenia gravis
- PMID: 12653847
- PMCID: PMC1808678
- DOI: 10.1046/j.1365-2249.2003.02113.x
Anti-cytokine autoantibodies in autoimmunity: preponderance of neutralizing autoantibodies against interferon-alpha, interferon-omega and interleukin-12 in patients with thymoma and/or myasthenia gravis
Abstract
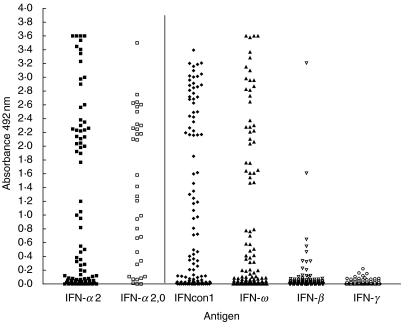
We have screened for spontaneous anticytokine autoantibodies in patients with infections, neoplasms and autoimmune diseases, because of their increasingly reported co-occurrence. We tested for both binding and neutralizing autoantibodies to a range of human cytokines, including interleukin-1alpha (IL-1alpha), IL-1beta, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12, IL-18, interferon-alpha2 (IFN-alpha2), IFN-omega, IFN-beta, IFN-gamma, tumour necrosis factor alpha (TNF-alpha), transforming growth factor beta-1 (TGF-beta1) and granulocyte-macrophage colony stimulating factor (GM-CSF), in plasmas or sera. With two notable exceptions described below, we found only occasional, mostly low-titre, non-neutralizing antibodies, mainly to GM-CSF; also to IL-10 in pemphigoid. Strikingly, however, high-titre, mainly IgG, autoantibodies to IFN-alpha2, IFN-omega and IL-12 were common at diagnosis in patients with late-onset myasthenia gravis (LOMG+), thymoma (T) but no MG (TMG-) and especially with both thymoma and MG together (TMG+). The antibodies recognized other closely related type I IFN-alpha subtypes, but rarely the distantly related type I IFN-beta, and never (detectably) the unrelated type II IFN-gamma. Antibodies to IL-12 showed a similar distribution to those against IFN-alpha2, although prevalences were slightly lower; correlations between individual titres against each were so modest that they appear to be entirely different specificities. Neither showed any obvious correlations with clinical parameters including thymoma histology and HLA type, but they did increase sharply if the tumours recurred. These antibodies neutralized their respective cytokine in bioassays in vitro; although they persisted for years severe infections were surprisingly uncommon, despite the immunosuppressive therapy also used in most cases. These findings must hold valuable clues to autoimmunizing mechanisms in paraneoplastic autoimmunity.
Figures




References
-
- Coutinho A, Kazatchkine MD, Avrameas S. Natural autoantibodies. Curr Opin Immunol. 1995;7:812–8. - PubMed
-
- Kotzin B. Systemic lupus erythematosus. Cell. 1996;85:303–6. - PubMed
-
- Song YH, Li Y, Maclaren NK. The nature of autoantigens targeted in autoimmune endocrine diseases. Immunol Today. 1996;17:232–8. - PubMed
-
- De Baets M. Autoimmune diseases against cell surface receptors: myasthenia gravis, a prototype anti-receptor disease. Neth J Med. 1994;45:294–301. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
