

Cytogenetic profile of unknown primary tumors: clues for their pathogenesis and clinical management
- PMID: 12659667
- PMCID: PMC1502119
- DOI: 10.1016/s1476-5586(03)80014-3
Cytogenetic profile of unknown primary tumors: clues for their pathogenesis and clinical management
Abstract
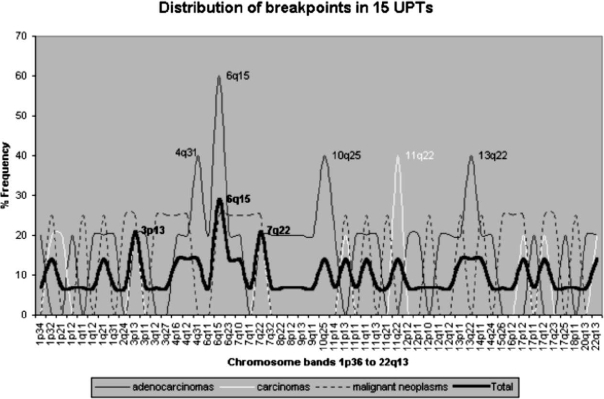
Unknown primary tumors (UPTs) represent an entity of great clinical and biological interest, whose origin cannot be determined even after medical workup. To better understand their pathogenesis by outlining their genetic composition, 20 UPTs were investigated by G-banding, supplemented with Fluorescence In Situ Hybridization and Comparative Genomic Hybridization analyses. The data obtained were sufficient to reach a diagnosis in five cases-four lymphomas and one Ewing sarcoma-demonstrating that in a subset of UPTs, cytogenetics can be an adjunct for differential diagnosis. In the remaining 15 UPTs, an aggressive cytogenetic pattern was revealed. The most frequently rearranged chromosome regions were 1q21, 3p13, 6q15-23, 7q22, 11p12-5, and 11q14-24, pinpointing gene loci probably associated with the peculiar pathogenesis of UPTs. The preferential involvement of 4q31, 6q15, 10q25, and 13q22 in adenocarcinomas (whereas 11q22 is involved in the rest of the carcinomas)-in addition to the marked divergence in the mean average of chromosomal changes, 16 and 3, respectively-demonstrates genotypic differences between the two histologic subgroups. Furthermore, the significantly shorter survival in cases displaying massive chromosome changes compared with those having a few changes indicates that the cytogenetic pattern might be used as a tool to assess prognosis in UPTs, even without the detection of their primary site.
Figures





Similar articles
-
Molecular and cytogenetic studies in the diagnosis of patients with poorly differentiated carcinomas of unknown primary site.J Clin Oncol. 1995 Jan;13(1):274-82. doi: 10.1200/JCO.1995.13.1.274. J Clin Oncol. 1995. PMID: 7799031
-
DNA in situ hybridization (interphase cytogenetics) versus comparative genomic hybridization (CGH) in human cancer: detection of numerical and structural chromosome aberrations.Acta Histochem. 2000 Feb;102(1):85-94. doi: 10.1078/0065-1281-00540. Acta Histochem. 2000. PMID: 10726167
-
G-banding and molecular cytogenetic analyses of marginal zone lymphoma.Br J Haematol. 2005 Sep;130(6):890-901. doi: 10.1111/j.1365-2141.2005.05706.x. Br J Haematol. 2005. PMID: 16156859
-
Cytogenetic and molecular cytogenetic analysis of B cell chronic lymphocytic leukemia: specific chromosome aberrations identify prognostic subgroups of patients and point to loci of candidate genes.Leukemia. 1997 Apr;11 Suppl 2:S19-24. Leukemia. 1997. PMID: 9178833 Review.
-
[Molecular cytogenetic techniques and their application in clinical diagnosis].Med Wieku Rozwoj. 2004 Jan-Mar;8(1):7-24. Med Wieku Rozwoj. 2004. PMID: 15557693 Review. Polish.
Cited by
-
Metastases in the Absence of a Primary Tumor: Advances in the Diagnosis and Treatment of CUP Syndrome.Dtsch Arztebl Int. 2008 Oct;105(43):733-40. doi: 10.3238/arztebl.2008.0733. Epub 2008 Oct 24. Dtsch Arztebl Int. 2008. PMID: 19623297 Free PMC article.
-
Carcinoma of unknown primary origin.Gastrointest Cancer Res. 2007 Nov;1(6):229-35. Gastrointest Cancer Res. 2007. PMID: 19262901 Free PMC article.
-
A review of the past, present, and future directions of neoplasia.Neoplasia. 2005 Dec;7(12):1039-46. doi: 10.1593/neo.05793. Neoplasia. 2005. PMID: 16354585 Free PMC article. Review. No abstract available.
-
A Systematic Review of Cancer of Unknown Primary in the Head and Neck Region.Cancer Manag Res. 2021 Sep 18;13:7235-7241. doi: 10.2147/CMAR.S319179. eCollection 2021. Cancer Manag Res. 2021. PMID: 34566429 Free PMC article. Review.
-
Cancer of Unknown Primary Site: Real Entity or Misdiagnosed Disease?J Cancer. 2020 Apr 6;11(13):3919-3931. doi: 10.7150/jca.42880. eCollection 2020. J Cancer. 2020. PMID: 32328196 Free PMC article. Review.
References
-
- Mackay B, Ordonez G. Pathologic evaluation of neoplasms with unknown primary site. Semin Oncol. 1993;20:206–228. - PubMed
-
- Abbruzzese JL, Raber MN. Unknown primary carcinoma. In: Abeloff MD, Armitage JO, Lichter AS, Niederhuber JE, editors. Clinical Oncology. New York: Churchill Livingstone; 1995. pp. 1833–1845.
-
- Hammar SP. Metastatic adenocarcinoma of unknown primary origin. Hum Pathol. 1998;29:1393–1402. - PubMed
-
- Lortholary A, Abadie-Lacourtoise S, Guerin O, Mege M, de Rauglaudre G, Gamelin E. Carcinoma of unknown primary site: 311 cases. Bull Cancer. 2001;88:619–627. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources