

Arrhythmogenic substrate of the pulmonary veins assessed by high-resolution optical mapping
- PMID: 12665495
- PMCID: PMC1995670
- DOI: 10.1161/01.CIR.0000058461.86339.7E
Arrhythmogenic substrate of the pulmonary veins assessed by high-resolution optical mapping
Abstract
Background: It has recently been recognized that atrial fibrillation can originate from focal sources in the pulmonary veins (PVs). However, the mechanisms of focal atrial fibrillation have not been well characterized. We assessed the electrophysiological characteristics of the PVs using high-resolution optical mapping.
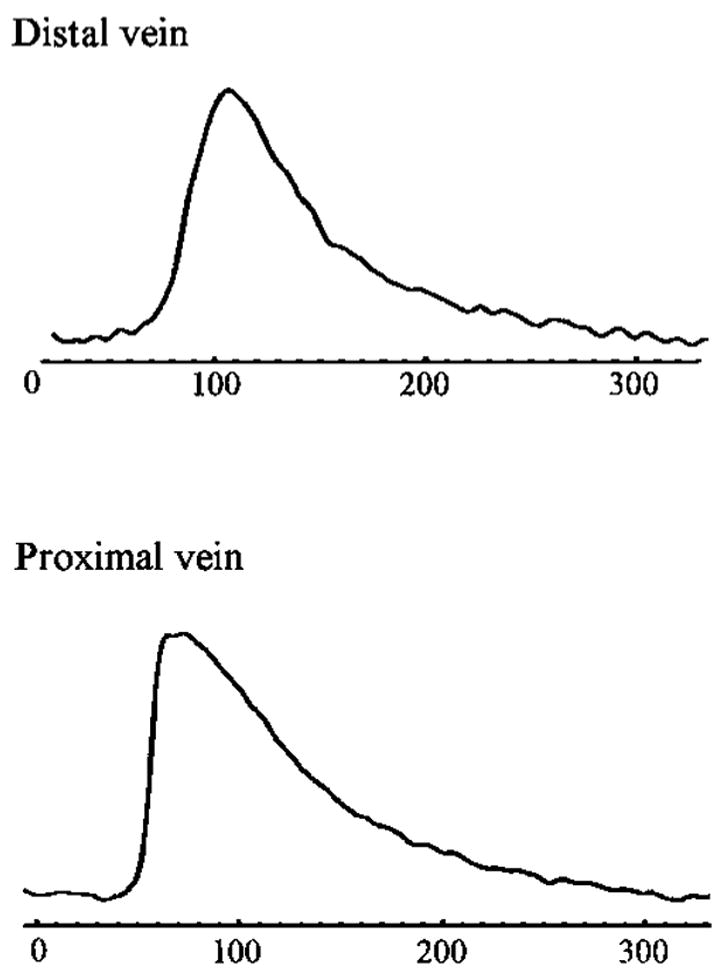
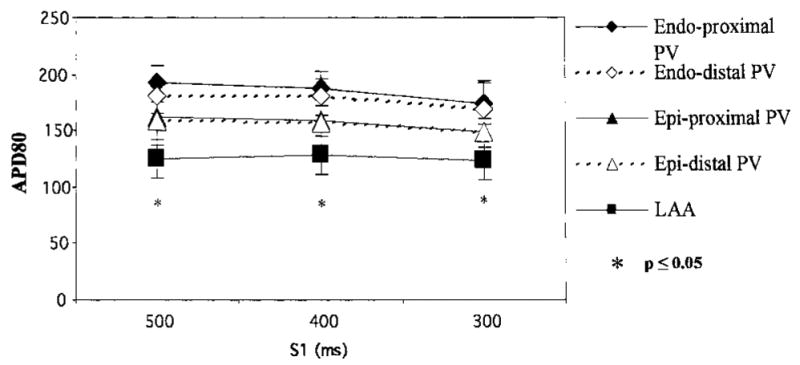
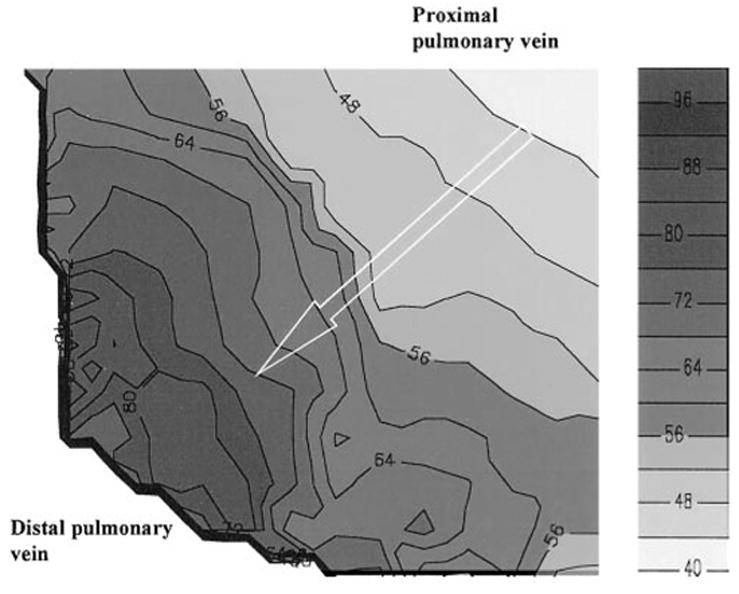
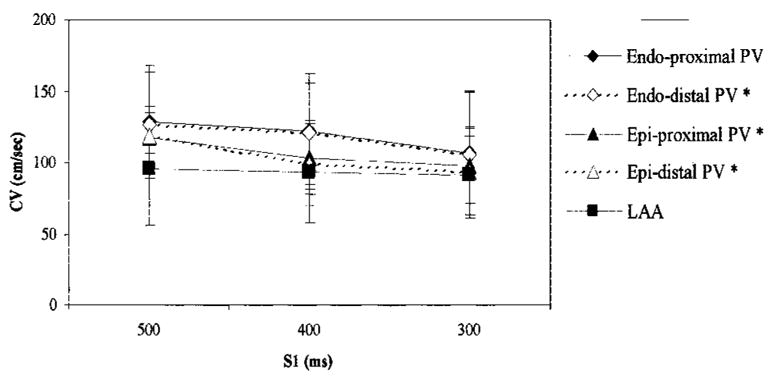
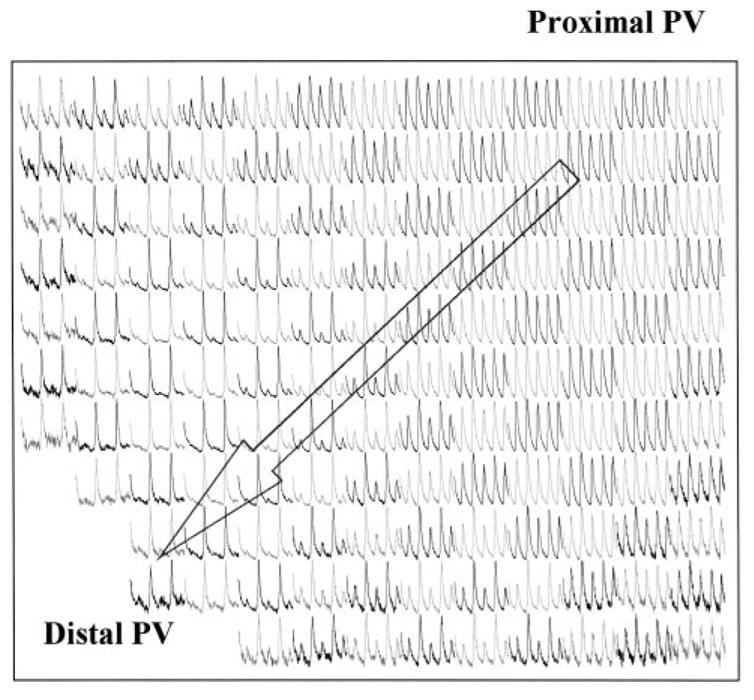
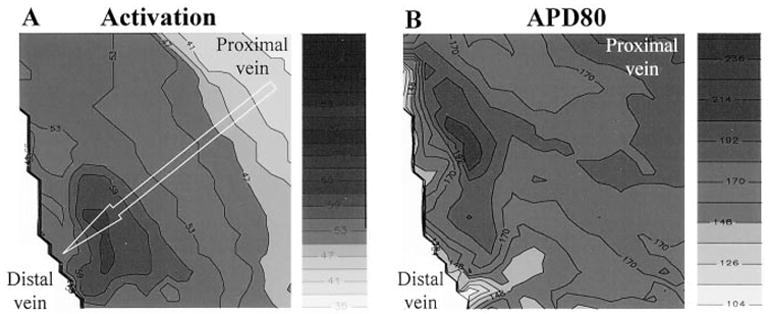
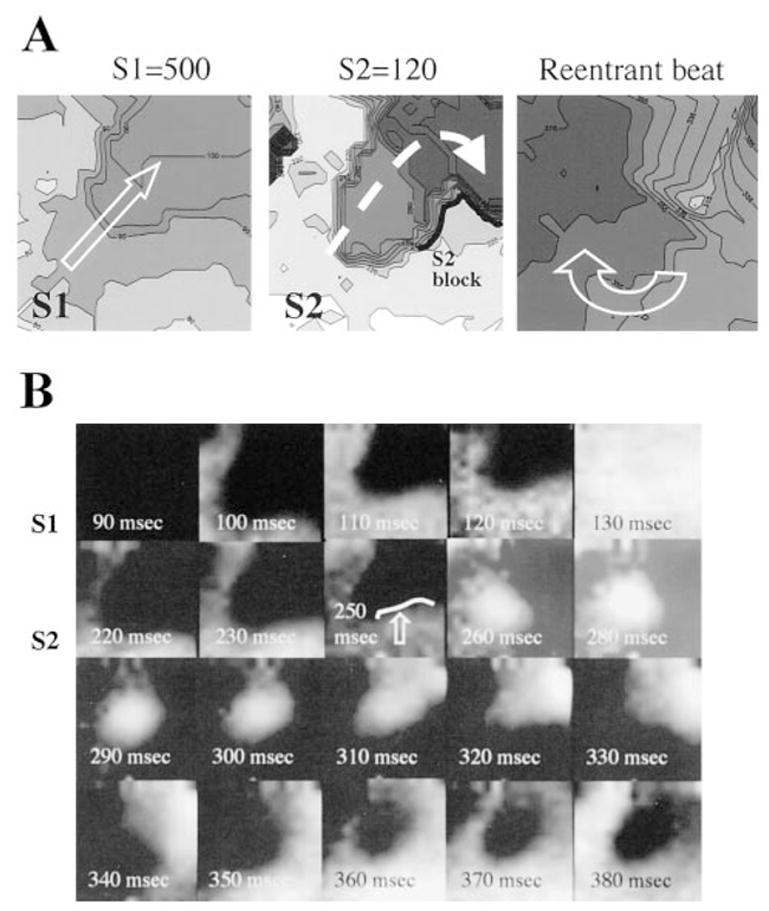
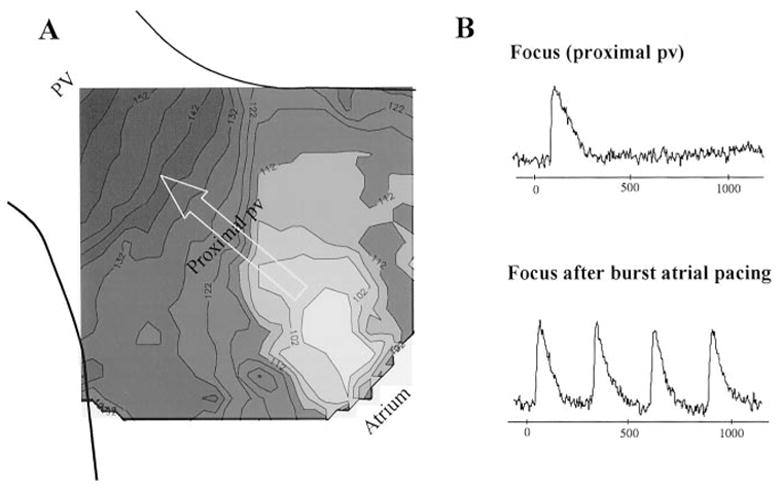
Methods and results: Coronary-perfused, isolated whole-atrial preparations from 33 normal dogs were studied. Programmed electrical stimulation was performed, and a 4-cm2 area of the PV underwent optical mapping of transmembrane voltage to obtain 256 simultaneous action potentials. Marked conduction slowing was seen at the proximal PV, compared with the rest of the vein, on both the epicardial (31.3+/-4.47 versus 90.2+/-20.7 cm/s, P=0.001) and endocardial (45.8+/-6.90 versus 67.6+/-10.4 cm/s, P=0.012) aspects. Pronounced repolarization heterogeneity was also noted, with action potential duration at 80% repolarization being longest at the PV endocardium. Nonsustained reentrant beats were induced with single extrastimuli, and the complete reentrant loop was visualized (cycle length, 155+/-30.3 ms); reentrant activity could be sustained with isoproterenol. Sustained focal discharge (cycle length, 330 to 1100 ms) was seen from the endocardial surface in the presence of isoproterenol; each focus was localized near the venous ostium.
Conclusions: The normal PV seems to have the necessary substrate to support reentry as well as focal activity. Although reentry occurred more distally in the vein, focal activity seemed to occur more proximally.
Figures
References
-
- Chen SA, Chiang CE, Yang CJ, et al. Sustained atrial tachycardia in adult patients. Electrophysiological characteristics, pharmacological response, possible mechanisms, and effects of radiofrequency ablation. Circulation. 1994;90:1262–1278. - PubMed
-
- Haissaguerre M, Jais P, Shah DC, et al. Catheter ablation of chronic atrial fibrillation targeting the reinitiating triggers. J Cardiovasc Electrophysiol. 2000;11:2–10. - PubMed
-
- Chen SA, Hsieh MH, Tai CT, et al. Initiation of atrial fibrillation by ectopic beats originating from the pulmonary veins: electrophysiological characteristics, pharmacological responses, and effects of radiofrequency ablation. Circulation. 1999;100:1879–1886. - PubMed
-
- Wu J, Olgin J, Miller JM, et al. Mechanisms underlying the reentrant circuit of atrioventricular nodal reentrant tachycardia in isolated canine atrioventricular nodal preparation using optical mapping. Circ Res. 2001;88:1189–1195. - PubMed
-
- Verheule S, Wilson E, Arora R, et al. Tissue structure and connexin expression of canine pulmonary veins. Cardiovasc Res. 2002;55:727–738. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
