

Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state
- PMID: 12668546
- PMCID: PMC151994
Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state
Erratum in
- CMAJ. 2003 May 13;168(10):1241
Abstract
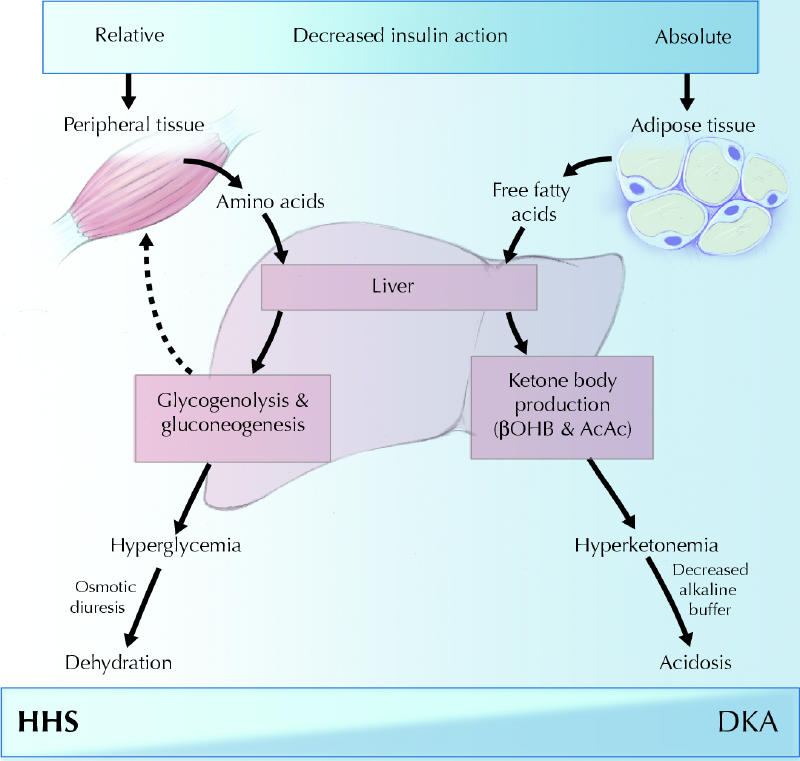
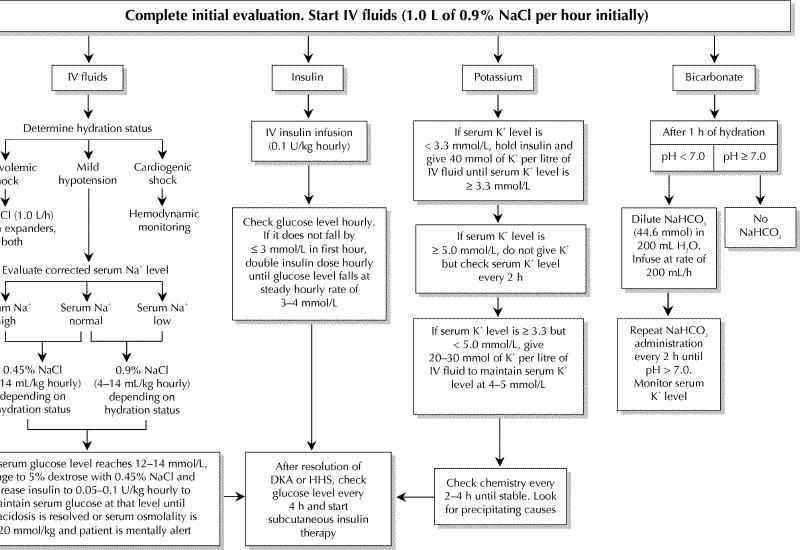
Diabetic ketoacidosis and the hyperglycemic hyperosmolar state are the most serious complications of diabetic decompensation and remain associated with excess mortality. Insulin deficiency is the main underlying abnormality. Associated with elevated levels of counterregulatory hormones, insulin deficiency can trigger hepatic glucose production and reduced glucose uptake, resulting in hyperglycemia, and can also stimulate lipolysis and ketogenesis, resulting in ketoacidosis. Both hyperglycemia and hyperketonemia will induce osmotic diuresis, which leads to dehydration. Clinical diagnosis is based on the finding of dehydration along with high capillary glucose levels with or without ketones in the urine or plasma. The diagnosis is confirmed by the blood pH, serum bicarbonate level and serum osmolality. Treatment consists of adequate correction of the dehydration, hyperglycemia, ketoacidosis and electrolyte deficits.
Figures
Comment in
-
CMAJ on the Web.CMAJ. 2003 Jun 10;168(12):1528. CMAJ. 2003. PMID: 12796328 Free PMC article. No abstract available.
-
Pediatric diabetic ketoacidosis.CMAJ. 2003 Aug 19;169(4):278-9; author reply 279. CMAJ. 2003. PMID: 12925411 Free PMC article. No abstract available.
References
-
- Ennis ED, Stahl E, Kreisberg RA. The hyperosmolar hyperglycemic syndrome. Diabetes Rev 1994;2:115-26.
-
- Fishbein H, Palumbo PJ. Acute metabolic complications in diabetes. In: National Diabetes Data Group. Diabetes in America. Bethesda (MD): National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 1995. p. 283-91.
-
- Choi BC, Shi F. Risk factors for diabetes mellitus by age and sex: results of the National Population Health Survey. Diabetologia 2001;44(10):1221-31. - PubMed
-
- Kitabchi AE, Wall BM. Diabetic ketoacidosis. Med Clin North Am 1995;79:9-37. - PubMed
-
- Foster DW, McGarry JD. The metabolic derangements and treatment of diabetic ketoacidosis. N Engl J Med 1983;309:159-69. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources