

Neoadjuvant systemic fluorouracil and mitomycin C prior to synchronous chemoradiation is an effective strategy in locally advanced rectal cancer
- PMID: 12671697
- PMCID: PMC2376366
- DOI: 10.1038/sj.bjc.6600822
Neoadjuvant systemic fluorouracil and mitomycin C prior to synchronous chemoradiation is an effective strategy in locally advanced rectal cancer
Abstract
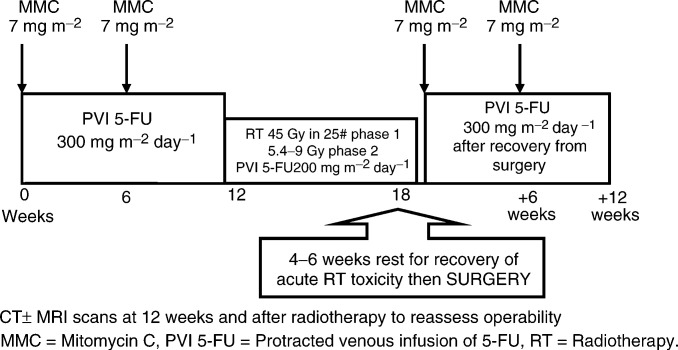
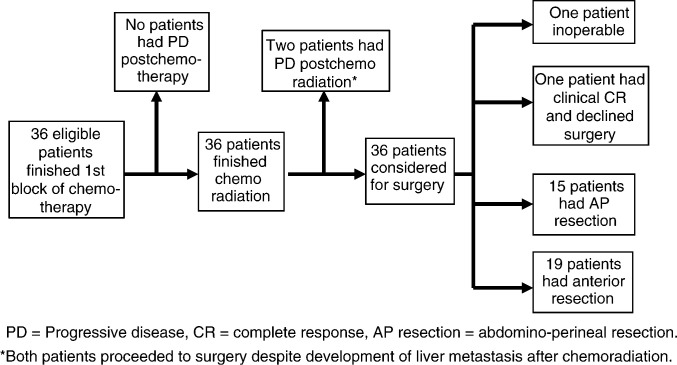
This study was designed to evaluate the benefits of neoadjuvant chemotherapy prior to chemoradiation and surgery in patients with locally advanced rectal cancer. Patients with previously untreated primary rectal cancer, reviewed in a multidisciplinary meeting and considered to have locally advanced disease on the basis of physical examination and imaging (MRI+CT n=30, CT alone n=6), were recruited. Patients received protracted venous infusion 5-FU (300 mg m(-2) day(-1) for 12 weeks) with mitomycin C (MMC) (7 mg m(-2) i.v. bolus every 6 weeks). Starting on week 13, 5-FU was reduced to 200 mg m(-2) day(-1) and concomitant pelvic radiotherapy 45 Gy in 25 fractions was commenced followed by 5.4-9 Gy boost to tumour bed. Surgery was planned 6 weeks after chemoradiation. Postoperatively, patients received 12 weeks of MMC and 5-FU at the same preoperative doses. Between January 99 and August 01, 36 eligible patients were recruited. Median age was 63 years (range=40-85). Following neoadjuvant chemotherapy, radiological tumour response was 27.8% (one CR and nine PRs) and no patient had progressive disease. In addition, 65% of patients had a symptomatic response including improvement in diarrhoea/constipation (59%), reduced rectal bleeding (60%) and diminished pelvic pain/tenesmus (78%). Following chemoradiation, tumour regression occurred in 80.6% (six CRs and 23 PRs; 95% CI=64-91.8%) and only one patient still had an inoperable tumour. R0 resection was achieved in 28 patients (82%). When compared with initial clinical staging, the pathological downstaging rate in T and/or N stage was 73.5% and pathological CR was found in one patient. Neoadjuvant systemic chemotherapy as a prelude to synchronous chemoradiation can be administered with negligible risk of disease progression and produces considerable symptomatic response with associated tumour regression.
Figures
References
-
- National Cancer Institute-Common Toxicity Criteria (1998) National Cancer Institute Bethesda http://ctep.cancer.gov/reporting/ctc.html
-
- Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, Johnston D, Dixon MF, Quirke P (1994) Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet 344: 707–711 - PubMed
-
- Aschele C, Friso ML, Pucciarelli S, Sartor L, Lonard S, De Salvo G, Fabris G, Da Dalt G, Ranzato R, Bruttocao A, Neri D, Finco C, Monfardini S (2002) A phase I–II study of weekly oxaliplatin, 5-fluorouracil continuous infusion and preoperative radiotherapy in locally advanced rectal cancer. Proc Am Soc Clin Oncol 21: 132a - PubMed
-
- Beets-Tan RG, Beets GL, Vliegen RF, Kessels AG, Van Boven H, De Bruine A, von Meyenfeldt MF, Baeten CG, van Engelshoven JM (2001) Accuracy of magnetic resonance imaging in prediction of tumour-free resection margin in rectal cancer surgery. Lancet 357: 497–504 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
