

Geographical inequalities in lung cancer management and survival in South East England: evidence of variation in access to oncology services?
- PMID: 12671698
- PMCID: PMC2376363
- DOI: 10.1038/sj.bjc.6600831
Geographical inequalities in lung cancer management and survival in South East England: evidence of variation in access to oncology services?
Erratum in
- Br J Cancer. 2004 Nov 15;91(10):1852
Abstract
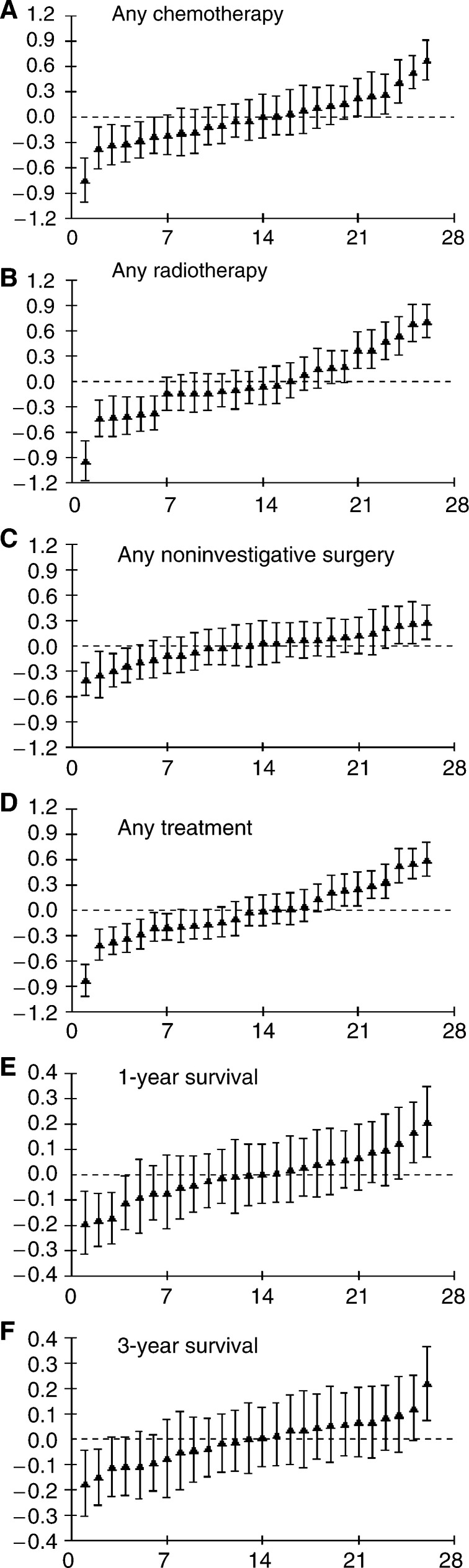
This study aimed to determine whether the management and survival of patients with lung cancer varied among 26 health authorities in South East England. The Thames Cancer Registry identified patients diagnosed with lung cancer (ICD-10 codes C33-C34) between 1995 and 1999. After excluding death certificate only patients, 32,818 (81%) patients were analysed. The proportions of patients receiving active treatment varied among health authorities between 5 and 17% for non-investigative surgery, 4 and 17% for any chemotherapy, 8 and 30% for any radiotherapy and 15 and 42% for any active treatment. One-year patient survival ranged from 11 to 34%. There was evidence of health authority level variation even after adjusting for case mix. Patients whose first hospital attendance was at a radiotherapy centre were more likely to receive active treatment (OR 1.72, 95% CI 1.21-2.46), chemotherapy (1.38, 1.06-1.79) or radiotherapy (1.86, 1.28-2.71). There was some evidence that patients whose first hospital attendance was at a radiotherapy centre survived longer. This study shows there is geographical inequality in the treatment given to lung cancer patients and patient survival in South East England. There was some evidence to suggest that these inequalities might be explained by variations in access to oncology services. Future studies should investigate the pathways and barriers to specialist care in this condition.
Figures
Similar articles
-
Variation in incidence of breast, lung and cervical cancer and malignant melanoma of skin by socioeconomic group in England.BMC Cancer. 2008 Sep 26;8:271. doi: 10.1186/1471-2407-8-271. BMC Cancer. 2008. PMID: 18822122 Free PMC article.
-
Explaining inequalities in access to treatment in lung cancer.J Eval Clin Pract. 2006 Oct;12(5):573-82. doi: 10.1111/j.1365-2753.2006.00644.x. J Eval Clin Pract. 2006. PMID: 16987120
-
Variation, precision and validity of 1-year survival estimates for lung, breast, colon and prostate cancer in South East England primary care trusts.Public Health. 2012 Jan;126(1):57-63. doi: 10.1016/j.puhe.2011.09.009. Epub 2011 Dec 6. Public Health. 2012. PMID: 22153886
-
Pulmonary resection after curative intent radiotherapy (>59 Gy) and concurrent chemotherapy in non-small-cell lung cancer.Ann Thorac Surg. 2004 Oct;78(4):1200-5; discussion 1206. doi: 10.1016/j.athoracsur.2004.04.085. Ann Thorac Surg. 2004. PMID: 15464470 Review.
-
Treatment disparities for disabled medicare beneficiaries with stage I non-small cell lung cancer.Arch Phys Med Rehabil. 2008 Apr;89(4):595-601. doi: 10.1016/j.apmr.2007.09.042. Arch Phys Med Rehabil. 2008. PMID: 18373987 Review.
Cited by
-
Barriers to lung cancer care: health professionals' perspectives.Support Care Cancer. 2017 Feb;25(2):497-504. doi: 10.1007/s00520-016-3428-3. Epub 2016 Oct 10. Support Care Cancer. 2017. PMID: 27726030 Free PMC article.
-
How do patient and hospital features influence outcomes in small-cell lung cancer in England?Br J Cancer. 2011 Sep 6;105(6):746-52. doi: 10.1038/bjc.2011.310. Epub 2011 Aug 9. Br J Cancer. 2011. PMID: 21829191 Free PMC article.
-
Epidemiological Study of Lung Cancer and Clinical Medication in England from 2001 to 2019.J Healthc Eng. 2022 Mar 23;2022:3577312. doi: 10.1155/2022/3577312. eCollection 2022. J Healthc Eng. 2022. Retraction in: J Healthc Eng. 2023 Oct 4;2023:9894620. doi: 10.1155/2023/9894620. PMID: 35368924 Free PMC article. Retracted.
-
Survival from lung cancer in England and Wales up to 2001.Br J Cancer. 2008 Sep 23;99 Suppl 1(Suppl 1):S43-6. doi: 10.1038/sj.bjc.6604584. Br J Cancer. 2008. PMID: 18813257 Free PMC article. No abstract available.
-
Variation in incidence of breast, lung and cervical cancer and malignant melanoma of skin by socioeconomic group in England.BMC Cancer. 2008 Sep 26;8:271. doi: 10.1186/1471-2407-8-271. BMC Cancer. 2008. PMID: 18822122 Free PMC article.
References
-
- Bach PB, Cramer LD, Schrag D, Downey RJ, Gelfand SE, Begg CB (2001) The influence of hospital volume on survival after resection for lung cancer. N Engl J Med 345: 181–188 - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, Brennan MF (1998) Impact of hospital volume on operative mortality for major cancer surgery. JAMA 280: 1747–1751 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
