

Rating the risk factors for breast cancer
- PMID: 12677142
- PMCID: PMC1514477
- DOI: 10.1097/01.SLA.0000059969.64262.87
Rating the risk factors for breast cancer
Abstract
Objective: To update and summarize evidence of risk factors for breast cancer.
Summary background data: Women who are at high risk for breast cancer have a variety of options available to them, including watchful waiting, prophylactic surgery, and chemoprevention. It is increasingly important to accurately assess a patient's risk profile to ensure that the cost/benefit ratio of the selected treatment is favorable.
Methods: Estimates of relative risk for documented risk factors were obtained from seminal papers identified in previous reviews. These estimates were updated where appropriate with data from more recent reports using large sample sizes or presenting meta-analyses of previous studies. These reports were identified from a review of the Medline database from 1992 to 2002.
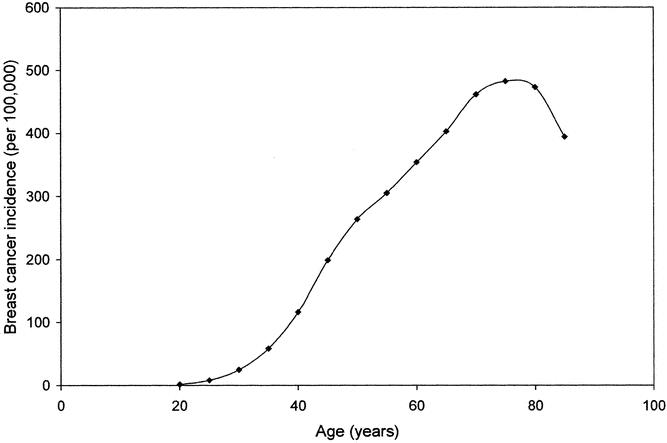
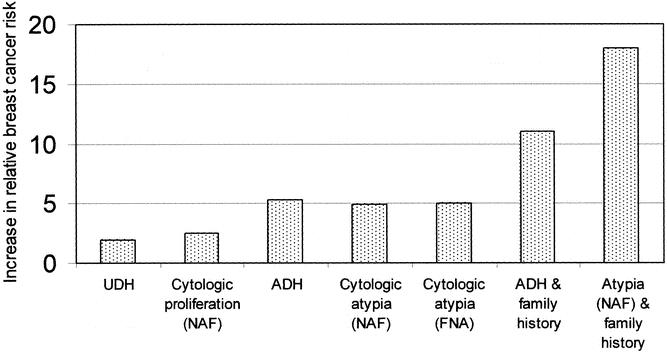
Results: Risk factors that have received a great deal of publicity (hormone use, alcohol consumption, obesity, nulliparity) present a relatively modest relative risk for breast cancer (<2). Factors associated with a prior history of neoplastic disease or atypical hyperplasia and factors associated with a genetic predisposition significantly affect the risk of breast cancer, with relative risks ranging from 3 (for some cases of positive family history) to 200 (for premenopausal women positive for a BRCA mutation).
Conclusions: More precise tools, based on techniques of molecular biology such as microarray analysis, will be needed to assess individual risk for breast cancer.
Figures
References
-
- Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998; 90: 1371–1388. - PubMed
-
- Ries LAG, Eisner MP, Kosary CL, et al. (eds). SEER Cancer Statistics Review, 1973–1997, National Cancer Institute. NIH Pub. No. 00–2789. Bethesda, MD, 2000.
-
- Vogel VG. Breast cancer risk factors and preventive approaches to breast cancer. In: Kavanagh JJ, Singletary SE, Einhorn N, et al. (eds). Cancer in women. Malden, MA: Blackwell Science, 1998: 58–91.
-
- Harvey EB, Schairer C, Brinton LA, et al. Alcohol consumption and breast cancer. J Natl Cancer Inst. 1987; 78: 657–661. - PubMed
-
- Manisto S, Virtanen M, Kataja V, et al. Lifetime alcohol consumption and breast cancer: a case-control study in Finland. Public Health Nutr. 2000; 3: 11–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
