

Curative potential of multimodality therapy for locally recurrent rectal cancer
- PMID: 12677146
- PMCID: PMC1514480
- DOI: 10.1097/01.SLA.0000059972.90598.5F
Curative potential of multimodality therapy for locally recurrent rectal cancer
Abstract
Objective: To assess the results of multimodality therapy for patients with recurrent rectal cancer and to analyze factors predictive of curative resection and prognostic for overall survival.
Summary background data: Locally recurrent rectal cancer is a difficult clinical problem, and radical treatment options with curative intent are not generally accepted.
Methods: A total of 394 patients underwent surgical exploration for recurrent rectal cancer. Ninety were found to have unresectable local or extrapelvic disease and 304 underwent resection of the recurrence. The latter patients were prospectively followed to determine long-term survival and factors influencing survival.
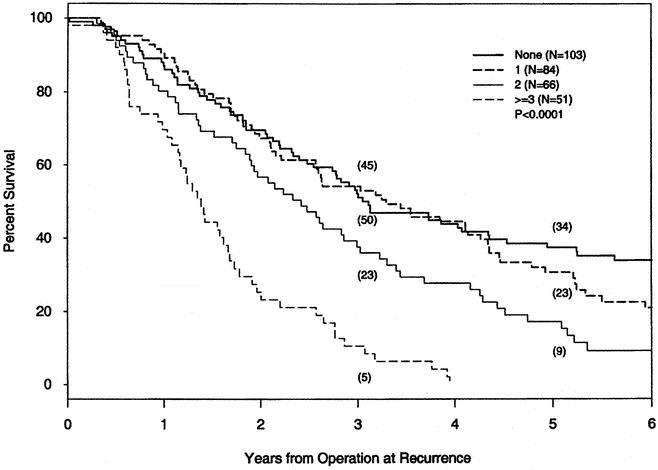
Results: Overall 5-year survival was 25%. Curative, negative resection margins were obtained in 45% of patients; in these patients a 5-year survival of 37% was achieved, compared to 16% (P <.001) in patients with either microscopic or gross residual disease. In a logistic regression analysis, initial surgery with end-colostomy and symptomatic pain (both univariate) and increasing number of sites of the recurrent tumor fixation in the pelvis (multivariate) were associated with palliative surgery. Overall survival was significantly decreased for symptomatic pain (P <.001) and more than one fixation (P =.029). Survival following extended resection of adjacent organs was not different from limited resection (28% vs. 21%, P =.11). Patient demographics and factors related to the initial rectal cancer did not affect outcome. Perioperative mortality was only 0.3%, but significant morbidity occurred in 26% of patients, with pelvic abscess being the most common complication.
Conclusions: This study demonstrates that many patients with locally recurrent rectal cancer can be resected with negative margins. Long-term survival can be achieved, especially for patients with no symptoms and minimal fixation of the recurrence in the pelvis, provided no gross residual disease remains.
Figures

References
-
- McCall JL, Cox MR, Wattchow DA. Analysis of local recurrence rates after surgery alone for rectal cancer. Int J Colorectal Dis. 1995; 10: 126–132. - PubMed
-
- Carlsson U, Lasson A, Ekelund G. Recurrence rates after curative surgery for rectal carcinoma, with special reference to their accuracy. Dis Colon Rectum. 1987; 30: 431–434. - PubMed
-
- Kramer T, Share R, Kiel K, et al. Intraoperative radiation therapy of colorectal cancer. In: Abe M, ed. Intraoperative radiation therapy. New York: Pergamon Press, 1991: 308–310.
-
- Cummings BJ, Rider WD, Harwood AR, et al. Radical external beam radiation therapy for adenocarcinoma of the rectum. Dis Colon Rectum. 1983; 26: 30–36. - PubMed
-
- Danjoux CE, Gelber RD, Catton GE, et al. Combination chemo-radiotherapy for residual, recurrent or inoperable carcinoma of the rectum: ECOG study (EST 3276). Int J Radiat Oncol Biol Phys. 1985; 11: 765–771. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
