

Usefulness of the pediatric electrocardiogram in detecting left ventricular hypertrophy: results from the Prospective Pediatric Pulmonary and Cardiovascular Complications of Vertically Transmitted HIV Infection (P2C2 HIV) multicenter study
- PMID: 12679770
- PMCID: PMC4417742
- DOI: 10.1067/mhj.2003.15
Usefulness of the pediatric electrocardiogram in detecting left ventricular hypertrophy: results from the Prospective Pediatric Pulmonary and Cardiovascular Complications of Vertically Transmitted HIV Infection (P2C2 HIV) multicenter study
Abstract
Background: A shortcoming of the pediatric electrocardiogram (ECG) appears to be its inability to accurately detect left ventricular hypertrophy (LVH). This study prospectively assesses the usefulness of the pediatric ECG as a screening modality for LVH.
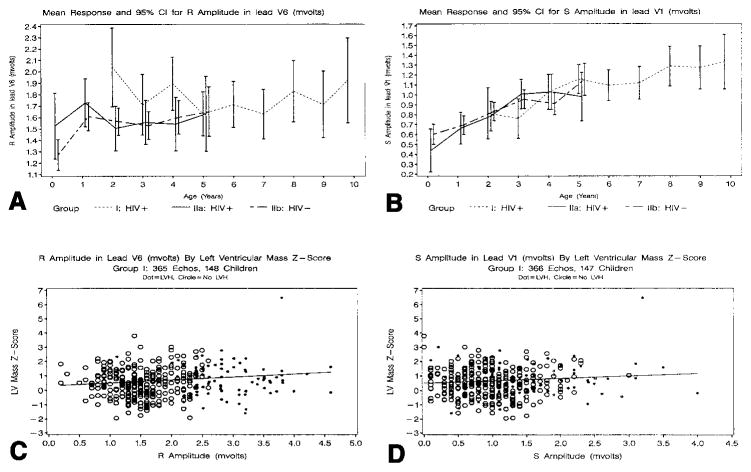
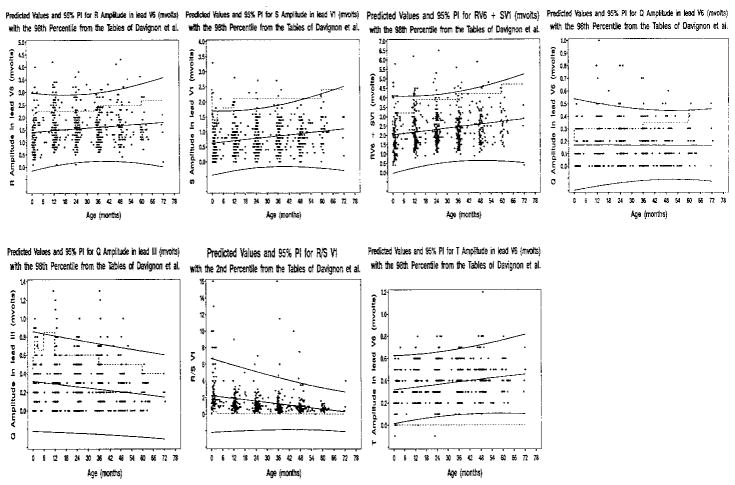
Methods: Concomitant echocardiograms and ECGs from a large cohort of children who were exposed to the human immunodeficiency virus (HIV; uninfected) and children who were infected with HIV were compared. By use of the values of Davignon et al, qualitative determination of LVH and quantitative criteria for LVH (RV6, SV1, RV6+SV1, QV6, and Q(III) >98% for age, R/SV1 <98% for age, and [-]TV6) were compared to body surface area adjusted for left ventricular (LV) mass z score. Results were then stratified according to weight and weight-for-height z scores. New age-adjusted predicted values were then constructed from children of a mixed race who were HIV-uninfected, < or =6 years old, and similarly assessed.
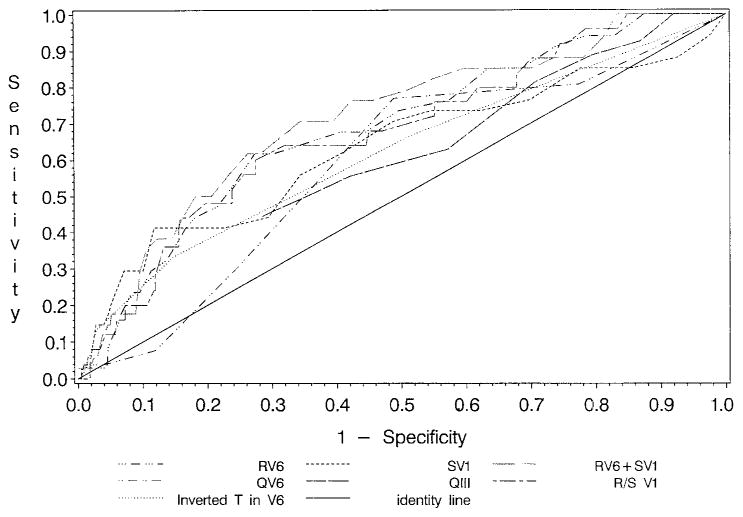
Results: The sensitivity rate was <20% for detecting increased LV mass, irrespective of HIV status; the specificity rate was 88% to 92%. The sensitivity rate of the individual criteria ranged from 0 to 35%; the specificity rate was 76% to 99%. Test sensitivities remained low when stratified by weight and weight-for-height z scores. Areas under the receiver operator characteristic curves were between 0.59 and 0.70, also suggesting poor accuracy of the ECG criteria. By use of new age-adjusted predicted values, the sensitivity rate decreased to <17%, and the specificity rate increased to 94% to 100%.
Conclusion: The ECG is a poor screening tool for identifying LVH in children. Sensitivity is not improved with revision of current criteria.
Figures
References
-
- Khan MN, Colan SD, Gamble W, et al. Diagnostic performance of electrocardiographic criteria for left ventricular hypertrophy in pediatric patients [abstract] Circulation. 1998;98:I-835.
-
- Devereux RB, Alonso DR, Lutas EM. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986;57:450–8. - PubMed
-
- Davignon A, Rautaharju P, Boiselle E, et al. Normal ECG standards for infants and children. Pediatr Cardiol. 1979;1:123–52.
Publication types
MeSH terms
Grants and funding
- K01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000645/RR/NCRR NIH HHS/United States
- RR-00043/RR/NCRR NIH HHS/United States
- N01-HR-96039/HR/NHLBI NIH HHS/United States
- N01-HR-96040/HR/NHLBI NIH HHS/United States
- RR-00071/RR/NCRR NIH HHS/United States
- M01 RR000865/RR/NCRR NIH HHS/United States
- M01 RR000533/RR/NCRR NIH HHS/United States
- N01 HR096037/HR/NHLBI NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- RR-00188/RR/NCRR NIH HHS/United States
- RR-00533/RR/NCRR NIH HHS/United States
- RR-00645/RR/NCRR NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- RR-00865/RR/NCRR NIH HHS/United States
- N01-HR-96042/HR/NHLBI NIH HHS/United States
- N01-HR-96038/HR/NHLBI NIH HHS/United States
- N01-HR-96041/HR/NHLBI NIH HHS/United States
- N01 HR096043/HR/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
