

Right trisectionectomy for primary liver cancer
- PMID: 12679915
- PMCID: PMC4611433
- DOI: 10.3748/wjg.v9.i4.706
Right trisectionectomy for primary liver cancer
Abstract
Aim: To evaluate the value of right trisectionectomy, previously named right trisegmentectomy, in the treatment of primary liver cancer by summarizing our 13-year experience for this procedure.
Methods: Thirty three primary liver cancer patients undergoing right trisectionectomy from Apr. 1987 to Dec. 1999 were investigated retrospectively. The impacts in survival of patients by cancerous biological behavior, such as tumor thrombi and satellite nodules, were discussed respectively. All right trisectionectomies were performed under normothermic interruption of porta hepatis at single time. Ultrasonic dissector (CUSA system 200) was used in dissection of hepatic parenchyma from Nov. 1992, instead of finger fracture.
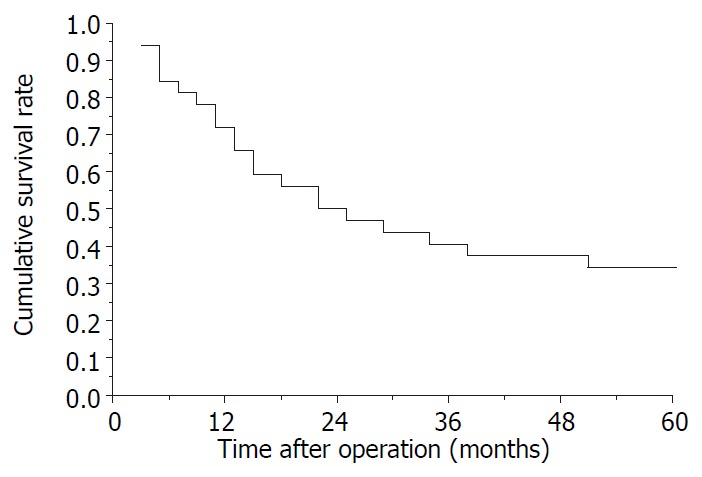
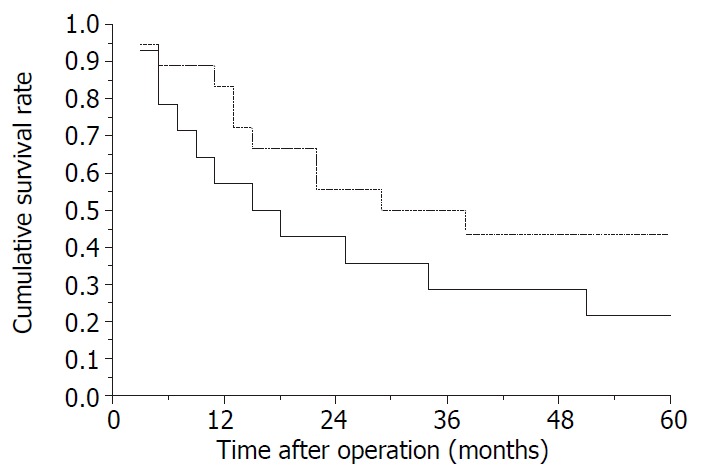
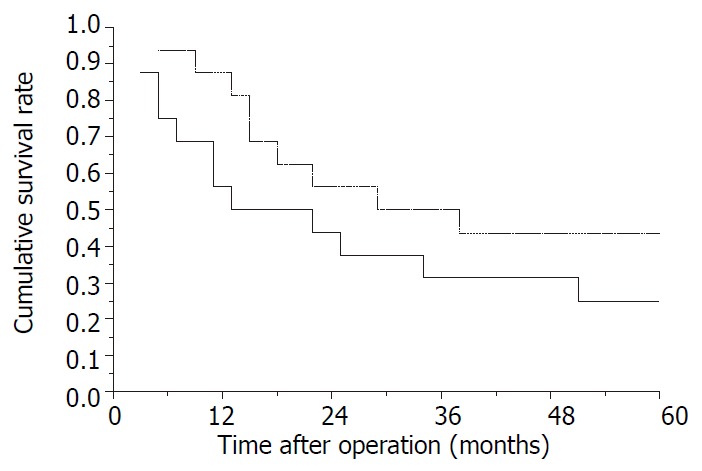
Results: 1-, 3- and 5-year survival rates were 71.9 %, 40.6 % and 34.4 %, respectively. The longest survival term with free cancer was 150 months (alive). There were no significant differences in survival curves between cases with and without tumor thrombi (right branch of portal vein) and satellite nodules. Operative mortality was 3.0 % (1/33). Main surgical complications occurred in 5 cases.
Conclusion: Right trisectionectomy should be regarded as an effective and safe procedure for huge primary liver cancers and is worth using more widely.
Figures
References
-
- Pisani P, Parkin DM, Bray F, Ferlay J. Estimates of the world-wide mortality from 25 cancers in 1990. Int J Cancer. 1999;83:18–29. - PubMed
-
- Makuuchi M, Takayama T, Kubota K, Kimura W, Midorikawa Y, Miyagawa S, Kawasaki S. Hepatic resection for hepatocellular carcinoma -- Japanese experience. Hepatogastroenterology. 1998;45 Suppl 3:1267–1274. - PubMed
-
- Shen P, Hoffman A, Howerton R, Loggie BW. Cryosurgery of close or positive margins after hepatic resection for primary and metastatic hepatobiliary malignancies. Am Surg. 2002;68:695–703; discussion 703. - PubMed
-
- Pelletier G, Ducreux M, Gay F, Luboinski M, Hagege H, Dao T, Van Steenbergen W, Buffet C, Rougier P, Adler M, et al. Treatment of unresectable hepatocellular carcinoma with lipiodol chemoembolization: a multicenter randomized trial. Groupe CHC. J Hepatol. 1998;29:129–134. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
