

Experimental study on the feasibility and safety of radiofrequency ablation for secondary splenomagely and hypersplenism
- PMID: 12679939
- PMCID: PMC4611456
- DOI: 10.3748/wjg.v9.i4.813
Experimental study on the feasibility and safety of radiofrequency ablation for secondary splenomagely and hypersplenism
Abstract
Aim: To assess the feasibility and safety of radiofrequency ablation (RFA) in treatment of secondary splenomagely and hypersplenism.
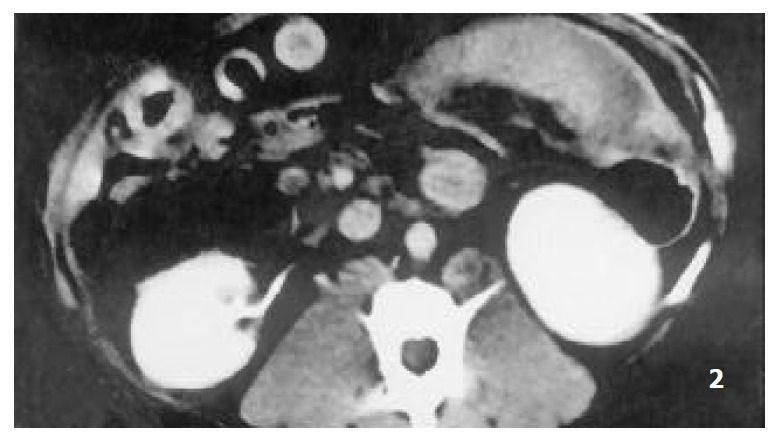
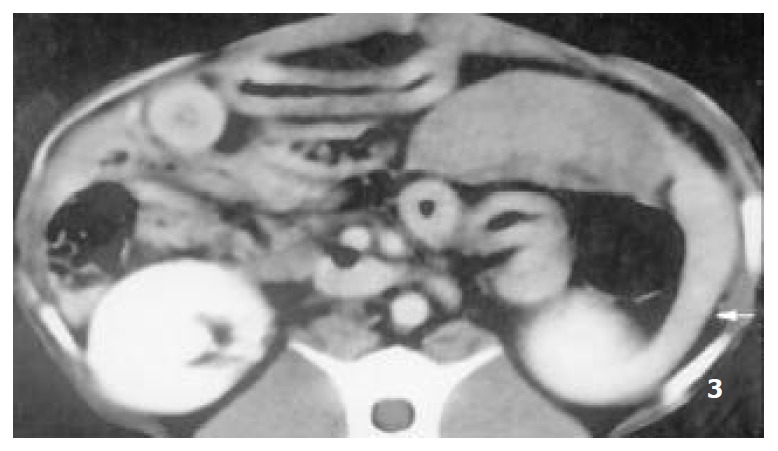
Methods: Sixteen healthy mongrel dogs were randomly divided into two groups, group I (n=4) and group II (n=12). Congestive splenomegaly was induced by ligation of splenic vein and its collateral branches in both groups. At the end of 3rd week postoperation, RFA in spleen was performed in group II via laparotomy, complications of RFA were observed, CT scan was performed and the spleens were obtained. The radiofrequency (RF) thermal lesions and histopathology of spleen were examined regularly.
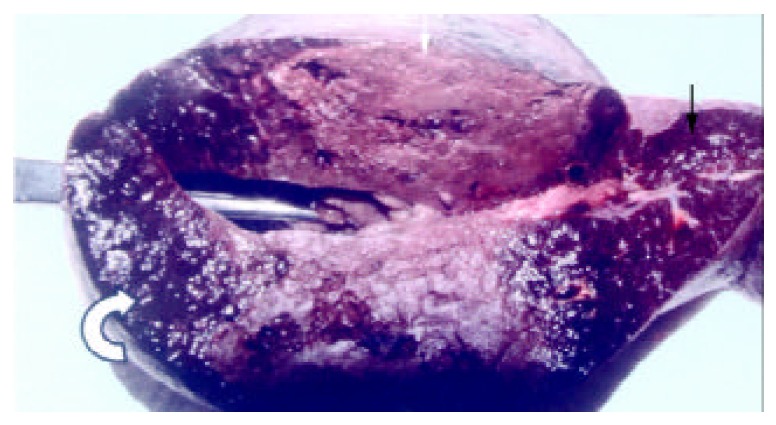
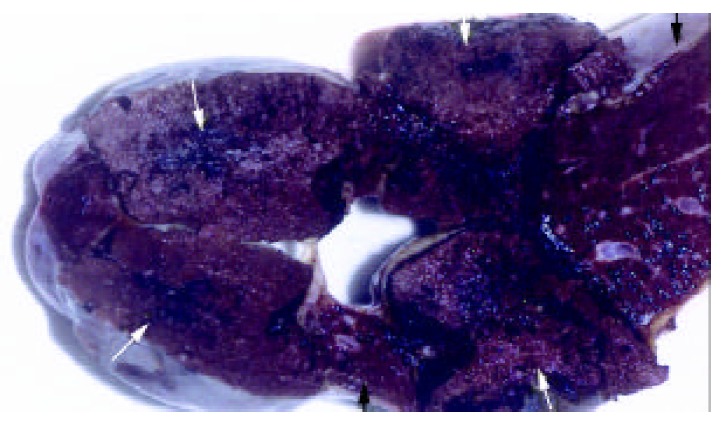
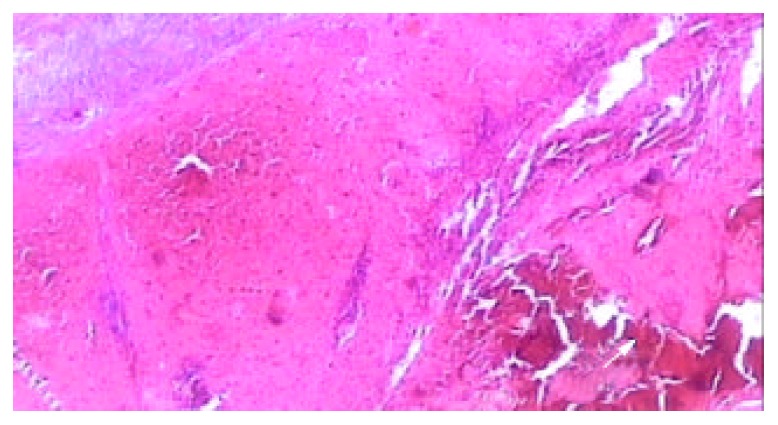
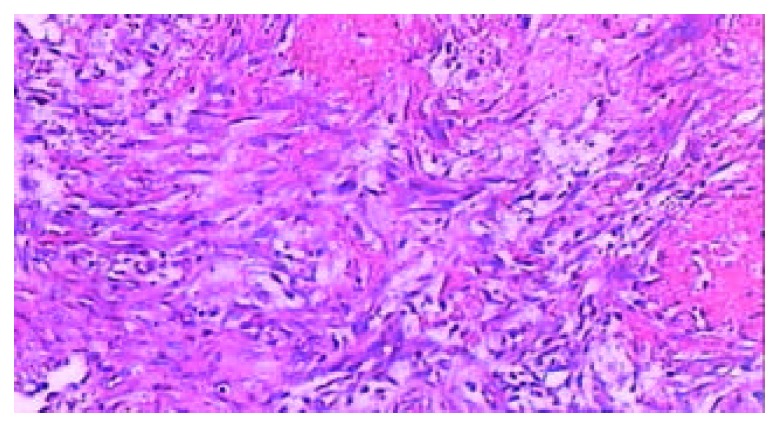
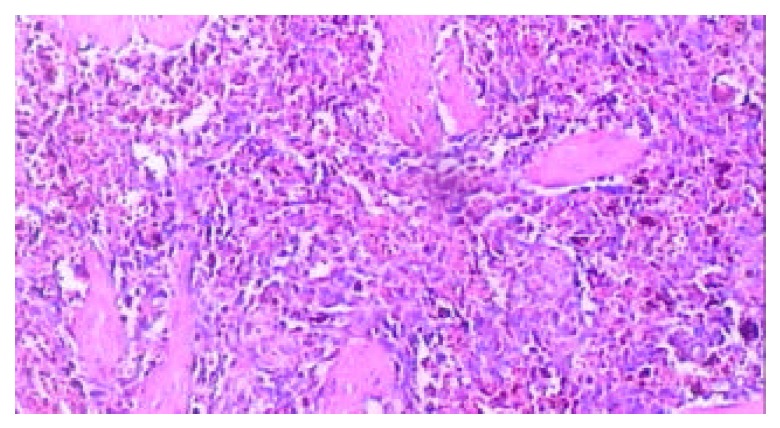
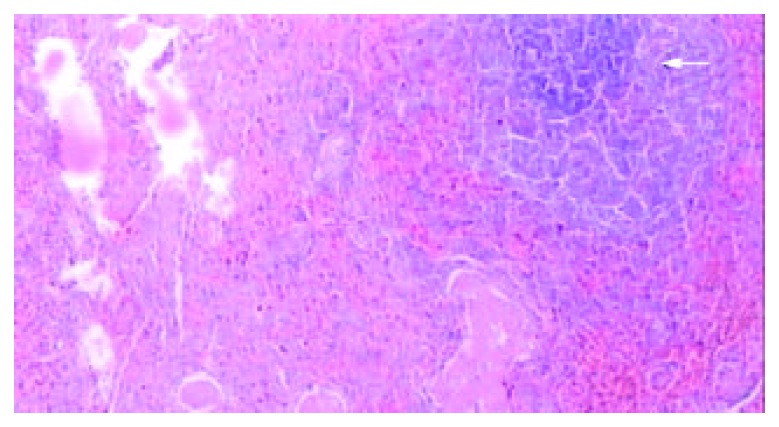
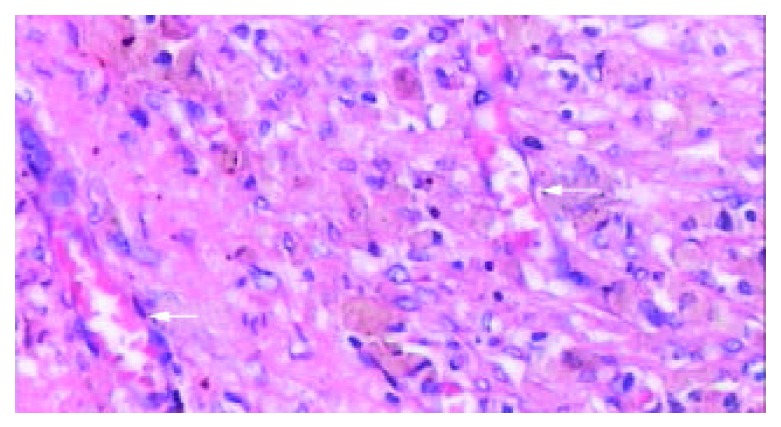
Results: No complication or death was observed in both groups; CT revealed that the splenomegaly lasted over 2 months after ligation of splenic vein; the segmental RF lesions included hyperintense zone of coagulative necrosis and more extensive peripheral hypointense infarcted zone, the latter was called "bystander effect". The infarcted zone would be absorbed and subsequently disappeared in 4-6 weeks after RFA accompanied with shrinkage of the remnant spleen. The fundamental histopathological changes of splenic lesions caused by RF thermal energy included local coagulative necrosis, peripheral thrombotic infarction zone, subsequent tissue absorption and fibrosis in the zone of thrombotic infarction, the occlusion of vessels in remnant viable spleen, deposition of extensive fibrous protein, and disappearance of congestive splenic sinusoid - "splenic carnification". Those pathologic changes were underline of shrinkage of spleen.
Conclusion: It is feasible and safe to perform RFA in spleen to treat experimental splenomegaly and hypersplenism. The RFA could be safely performed clinically via laparotomy or laparoscopic procedure while spleen was strictly separated from surrounding organs.
Figures

Similar articles
-
[The feasibility and safety of radiofrequency ablation for secondary splenomegaly and hypersplenism in dogs].Zhonghua Wai Ke Za Zhi. 2003 Apr;41(4):299-302. Zhonghua Wai Ke Za Zhi. 2003. PMID: 12882678 Chinese.
-
The effects of splenic artery ligation in an experimental model of secondary hypersplenism.J R Coll Surg Edinb. 2000 Jun;45(3):148-52. J R Coll Surg Edinb. 2000. PMID: 10881479
-
Preliminary experimental study on splenic hemodynamics of radiofrequency ablation for the spleen.Minim Invasive Ther Allied Technol. 2017 Aug;26(4):193-199. doi: 10.1080/13645706.2017.1281315. Epub 2017 Feb 1. Minim Invasive Ther Allied Technol. 2017. PMID: 28145148
-
Thermal ablation for partial splenectomy hemostasis, spleen trauma, splenic metastasis and hypersplenism.Hepatogastroenterology. 2013 May;60(123):501-6. doi: 10.5754/hge12853. Hepatogastroenterology. 2013. PMID: 23159352 Review.
-
A review of radiofrequency ablation: Large target tissue necrosis and mathematical modelling.Phys Med. 2016 Aug;32(8):961-71. doi: 10.1016/j.ejmp.2016.07.092. Epub 2016 Jul 25. Phys Med. 2016. PMID: 27461969 Review.
Cited by
-
Experimental study of destruction to porcine spleen in vivo by microwave ablation.World J Gastroenterol. 2011 Dec 7;17(45):5014-20. doi: 10.3748/wjg.v17.i45.5014. World J Gastroenterol. 2011. PMID: 22174552 Free PMC article.
-
Comparison of 3D ultrasound and magnetic resonance imaging for microwave ablation in the canine splenomegaly model.Int J Comput Assist Radiol Surg. 2015 Apr;10(4):459-64. doi: 10.1007/s11548-014-1095-8. Epub 2014 Jul 3. Int J Comput Assist Radiol Surg. 2015. PMID: 24989968
-
Radiofrequency ablation for hypersplenism in patients with liver cirrhosis: a pilot study.J Gastrointest Surg. 2005 May-Jun;9(5):648-57. doi: 10.1016/j.gassur.2004.11.006. J Gastrointest Surg. 2005. PMID: 15862259
-
A case of splenic abscess after radiofrequency ablation.World J Gastroenterol. 2006 Jul 14;12(26):4256-8. doi: 10.3748/wjg.v12.i26.4256. World J Gastroenterol. 2006. PMID: 16830388 Free PMC article.
-
Hepatectomy combined with microwave ablation of the spleen for treatment of hepatocellular carcinoma complicated with splenomegaly: A retrospective study.Mol Clin Oncol. 2017 Feb;6(2):204-208. doi: 10.3892/mco.2016.1111. Epub 2016 Dec 14. Mol Clin Oncol. 2017. PMID: 28357095 Free PMC article.
References
-
- Ma K, Min C, Ian HX, Jiahong D. Prevention and cure of complications from multiple-electrode radiofrequency treatment of liver tumors. Dig Dis. 2001;19:364–366. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
