

Undertreatment of hypercholesterolaemia: a population-based study
- PMID: 12680888
- PMCID: PMC1884230
- DOI: 10.1046/j.1365-2125.2003.01769.x
Undertreatment of hypercholesterolaemia: a population-based study
Abstract
Aims: To assess the level of undertreatment of hypercholesterolaemia in the general population, taking intra-person variability in serum cholesterol concentrations into account, and to identify determinants of undertreatment of hypercholesterolaemia.
Methods: In this cross-sectional study, data from two population-based surveys on cardiovascular disease risk factors conducted between 1987 and 1997 in the Netherlands were used. For all 64 757 respondents aged 20-59 years, treatment eligibility for lipid-lowering drug use was established according to the Dutch Cholesterol Consensus. Multivariate logistic models were used to identify determinants of undertreatment.
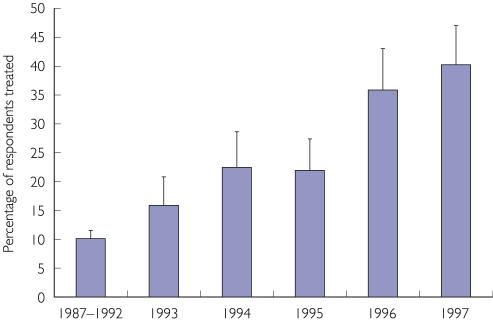
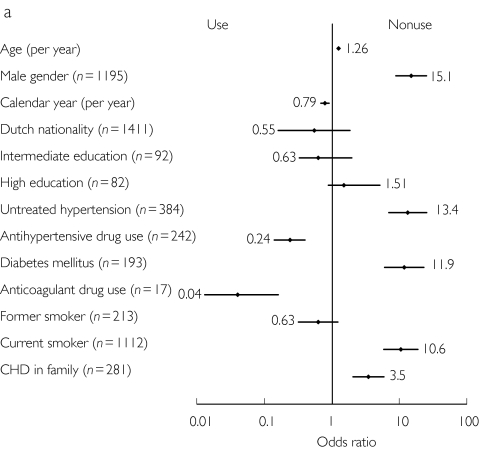
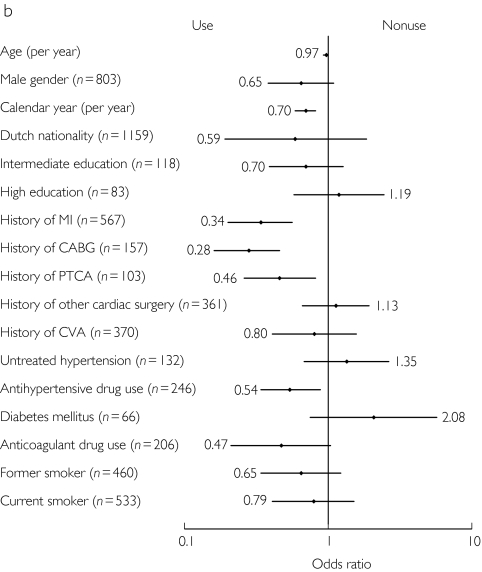
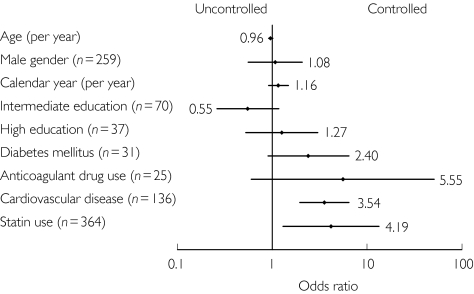
Results: During the study period, 56.8% of the study population had undesirable cholesterol concentrations (serum total cholesterol> 5 mmol l(-1)) and 5.5% of those were eligible for pharmacological treatment based on their absolute risk of coronary heart disease. Of those eligible for pharmacological treatment, 16.3% were treated, and 19.6% of those treated had their serum total cholesterol concentration controlled. Only 3.2% of those eligible for pharmacological treatment were both treated and controlled. We identified several determinants for undertreatment, e.g. male gender and younger age for primary prevention and female gender and older age for secondary prevention. Treatment has improved slightly in more recent years.
Conclusions: Over 95% of the population eligible for the pharmacological treatment of hypercholesterolaemia was either untreated or was uncontrolled. To decrease undertreatment, identification of high-risk patients should be increased. Those who are treated with lipid-lowering medication could further benefit from more aggressive treatment, especially with statins.
Figures
References
-
- Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med. 1995;333:1301–1307. - PubMed
-
- Downs JR, Clearfield M, Weis S, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279:1615–1622. - PubMed
-
- Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S) Lancet. 1994;344:1383–1389. - PubMed
-
- Sacks FM, Pfeffer MA, Moye LA, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med. 1996;335:1001–1009. - PubMed
-
- The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–1357. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
