

Cancer in pregnancy: maternal-fetal conflict
- PMID: 12684890
- PMCID: PMC12161954
- DOI: 10.1007/s00432-002-0406-6
Cancer in pregnancy: maternal-fetal conflict
Abstract
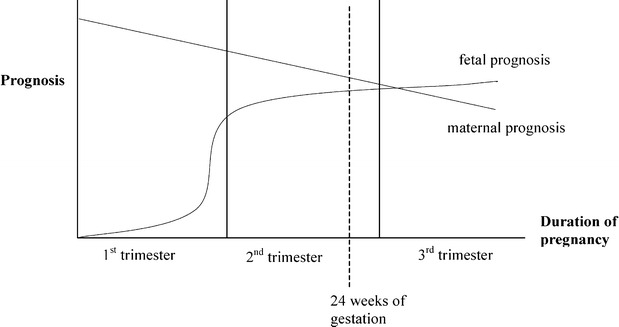
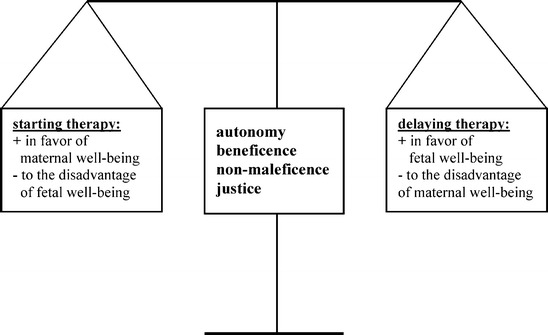
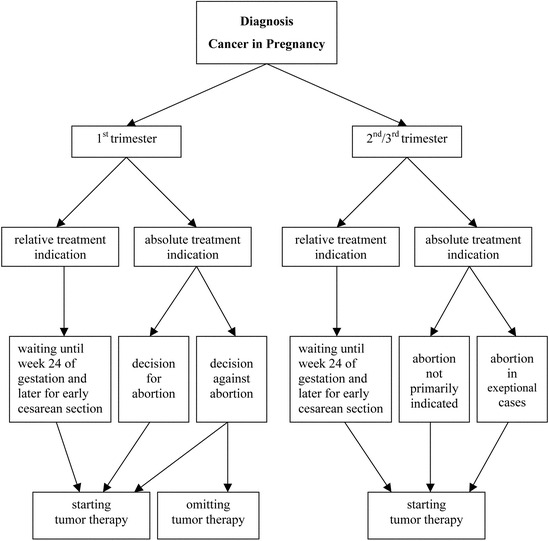
The occurrence of malignancies during pregnancy has increased over the last decades. They complicate approximately 1 per 1000 pregnancies. The most common malignancies associated with pregnancy include malignant melanoma, malignant lymphomas and leukemia, and cancer of the cervix, breast, ovary, colon and thyroid. Since it is impossible for prospective randomized clinical trials to be conducted in this field, relevant data have been generated from case reports and matched historical cohort studies in order to evaluate the treatment outcomes and the issues complicating the management of malignancy in the pregnant patient. There is almost always a conflict between optimal maternal therapy and fetal well-being. The maternal interest is for an immediate treatment of the recently diagnosed tumor. However, the optimal therapy, be it chemotherapy, radiotherapy or surgery, may impose great risks on the fetus. Consequently, either maternal or fetal health, or both, will be compromised. Therefore, both the pregnant patient and her physician are often in a dilemma as to the optimal course. On the basis of the medical facts, we discuss the issues raising potential ethical conflicts and present a practical ethical approach which may help to increase clarity in maternal-fetal conflicts. We review the available data informing the incidence and impact of the most common malignancies during pregnancy and their treatment on both the pregnant woman and her fetus. The optimal therapy for the tragic diagnosis of cancer in pregnancy requires a collaborative and interdisciplinary approach between gynecologists, oncologists, obstetricians, surgeons, neonatologists, psychologists, nursing staff and other disciplines. The purpose of this article is not to answer specific questions or to construct management schemes for specific tumors but to provide a framework for approaching some of these complex issues.
Figures
References
-
- Adami HO, Tsaih S, Lambe M, et al (1993) Pregnancy and risk of non-Hodgkin's lymphoma: a prospective study. Int J Cancer 70:155–158 - PubMed
-
- Allen HH, Nisker JA (1986) Cancer in pregnancy. Futura Publishing, New York, p 3
-
- Alothman A, Sparling TG (1994) Managing hairy cell leukemia in pregnancy (letter). Ann Intern Med 120:1048–1049 - PubMed
-
- Antonelli NM, Dotters DJ, Katz VL, Kuller JA (1996) Cancer in pregnancy: a review of the literature. Part I and II. Obstet Gynecol Surv 51:125–142 - PubMed
-
- Atar E, Dgani R, Shoham Z, Bornstein R (1990) Ovarian cancer during pregnancy. Harefuah 119:146–148 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
