

Interleukin-2 receptor monoclonal antibodies in renal transplantation: meta-analysis of randomised trials
- PMID: 12689974
- PMCID: PMC153097
- DOI: 10.1136/bmj.326.7393.789
Interleukin-2 receptor monoclonal antibodies in renal transplantation: meta-analysis of randomised trials
Abstract
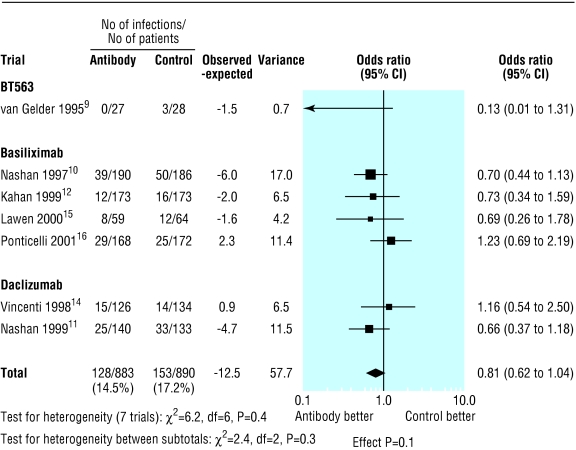
Objective: To study the effect of interleukin-2 receptor monoclonal antibodies on acute rejection episodes, graft loss, deaths, and rate of infection and malignancy in patients with renal transplants.
Design: Meta-analysis of published data.
Data sources: Medline, Embase, and Cochrane library for years 1996-2003 plus search of medical editors' trial amnesty and contact with manufacturers of the antibodies.
Selection of studies: Randomised controlled trials comparing interleukin-2 receptor antibodies with placebo or no additional treatment in patients with renal transplants receiving ciclosporin based immunosuppression.
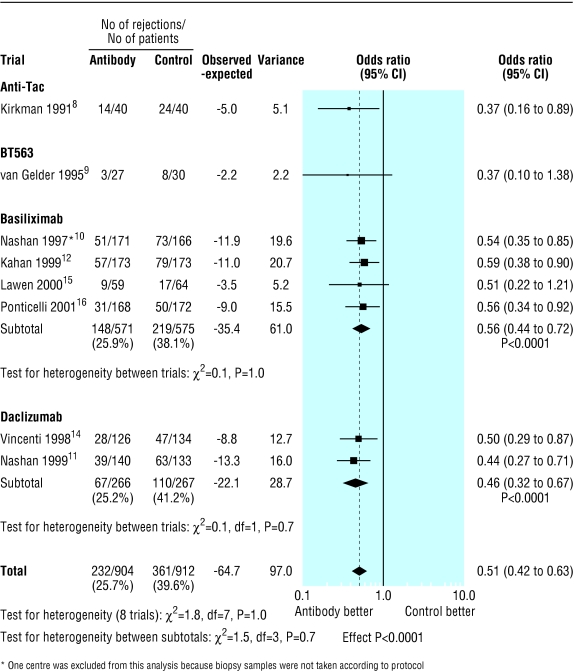
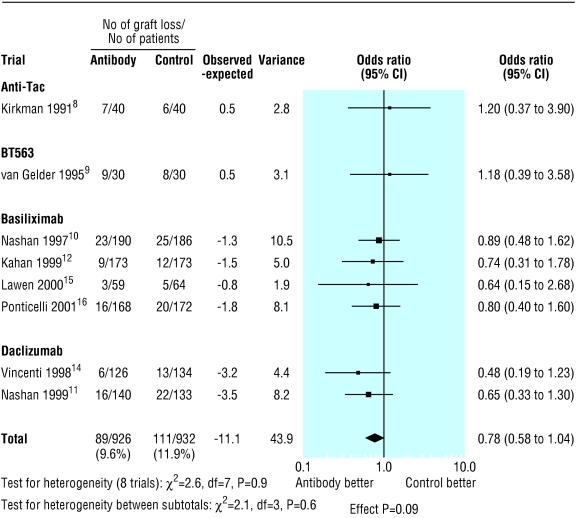
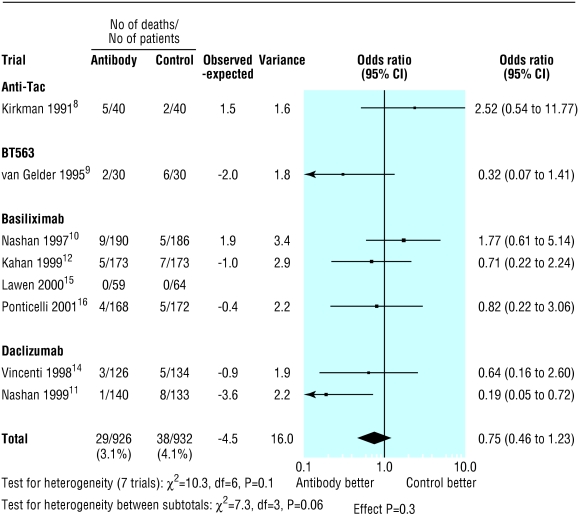
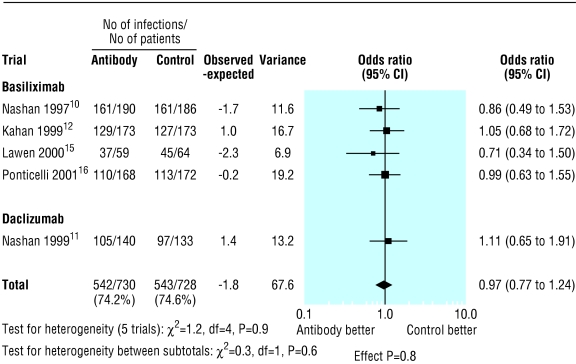
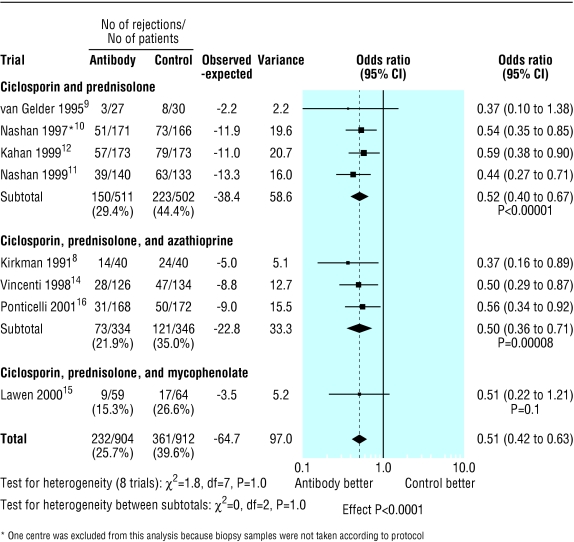
Results: Eight randomised controlled trials involving 1871 patients met the selection criteria (although only 1858 patients were analysed). Interleukin-2 receptor antibodies significantly reduced the risk of acute rejection (odds ratio 0.51, 95% confidence interval 0.42 to 0.63). There were no significant differences in the rate of graft loss (0.78, 0.58 to 1.04), mortality (0.75, 0.46 to 1.23), overall incidence of infections (0.97, 0.77 to 1.24), incidence of cytomegalovirus infections (0.81, 0.62 to 1.04), or risk of malignancies at one year (0.82, 0.39 to 1.70). The different antibodies had a similar sized effect on acute rejection (test for heterogeneity P=0.7): anti-Tac (0.37, 0.16 to 0.89), BT563 (0.37, 0.1 to 1.38), basiliximab (0.56, 0.44 to 0.72), and daclizumab (0.46, 0.32 to 0.67). The reduction in acute rejections was similar for all ciclosporin based immunosuppression regimens (test for heterogeneity P=1.0).
Conclusions: Adding interleukin-2 receptor antibodies to ciclosporin based immunosuppression reduces episodes of acute rejection at six months by 49%. There is no evidence of an increased risk of infective complications. Longer follow up studies are needed to confirm whether interleukin-2 receptor antibodies improve long term graft and patient survival.
Figures

References
-
- UK Transplant website. www.uktransplant.org (accessed 25 February 2003).
-
- Hariharan S, Johnson C, Bresnahan B, Taranto S, McIntosh M, Stablein D. Improved graft survival after renal transplantation in the United States, 1988 to 1996. N Engl J Med. 2000;342:605–612. - PubMed
-
- Matas A, Gillingham K, Payne W, Najarian J. The impact of an acute rejection episode on long-term renal allograft survival. Transplantation. 1994;57:857–859. - PubMed
-
- Kamel O, van de Rijn M, Lebrun D, Weiss L, Warnke R, Dorfman R. A multivariate analysis of discharge immunosuppression and post-transplant malignancy. Am J Transplant. 2001;1(suppl 1):353.
-
- Jamil B, Nicholls K, Becker G, Walker R. Impact of acute rejection therapy on infections and malignancies in renal transplant recipients. Transplantation. 1999;68:1597–1619. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous