

Chromosome 4 hyperploidy represents an early genetic aberration in premalignant Barrett's oesophagus
- PMID: 12692043
- PMCID: PMC1773637
- DOI: 10.1136/gut.52.5.623
Chromosome 4 hyperploidy represents an early genetic aberration in premalignant Barrett's oesophagus
Abstract
Background and aims: Characterisation of the underlying molecular mechanisms that promote Barrett's progression may ultimately lead to identification of potential predictive genetic markers that classify patients' malignant risk. In an attempt to understand these causative pathways, fluorescence in situ hybridisation (FISH) was used in this study to determine when specific genetic alterations arise during Barrett's associated neoplastic progression.
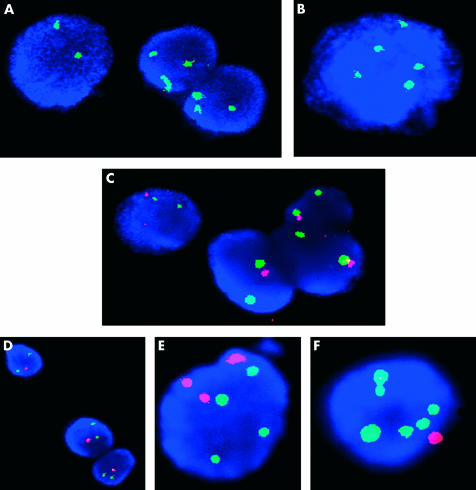
Methods: Endoscopic cytology brushings were obtained from 28 patients with Barrett's metaplasia, 28 with dysplasia (20 low grade dysplasia (LGD) and eight with high grade dysplasia (HGD)), and seven with adenocarcinoma, together with paired control brushings from regions of normal proximal squamous cell epithelium. The exfoliated epithelial cells were washed and deposited onto slides. Probes specific for the centromeres of chromosomes 4, 8, 20, and Y, and locus specific probes for the tumour suppressor genes p16, p53, and Rb were subsequently hybridised.
Results: Aneuploidy was found early in progression, with metaplastic tissues displaying increased copy numbers of chromosomes 4 and 8. Chromosome 4 hyperploidy was found in 89%, 90%, 88%, and 100% of metaplasias, LGD, HGD, adenocarcinomas, respectively, while chromosome 8 hyperploidy occurred in 71%, 75%, 100%, and 100% of patients with the respective staging. Loss of the p16 tumour suppressor gene also presented in metaplastic epithelium (7%) but most other genetic aberrations were only seen in HGD.
Conclusions: Genetic instability arises well before dysplasia in Barrett's oesophagus, with chromosome 4 and 8 hyperploidy representing the earliest and most common alterations identified. As these aberrations are widespread at all the premalignant stages, there may be genes on chromosomes 4 and 8 that are involved in both the initiation and progression of Barrett's oesophagus.
Figures

References
-
- Lagergren J, Bergstrom R, Lindgren A, et al. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999;340:825–31. - PubMed
-
- Sampliner RE. Practice guidelines on the diagnosis, surveillance, and therapy of Barrett’s esophagus. Am J Gastroenterol 1998;93:1028–31. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83:2049–53. - PubMed
-
- Solaymani Dodaran M, Silcocks PB, Logan RFA. Continuing rise in incidence of oesophageal adenocarcinoma in England and Wales. Gut 2001;48(suppl 1):110. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous