

Progressive sclerosing cholangitis after septic shock: a new variant of vanishing bile duct disorders
- PMID: 12692054
- PMCID: PMC1773636
- DOI: 10.1136/gut.52.5.688
Progressive sclerosing cholangitis after septic shock: a new variant of vanishing bile duct disorders
Abstract
Background: We present nine patients with progressive sclerosing cholangitis after septic shock.
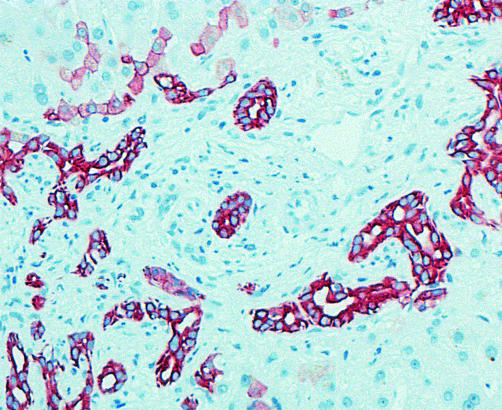
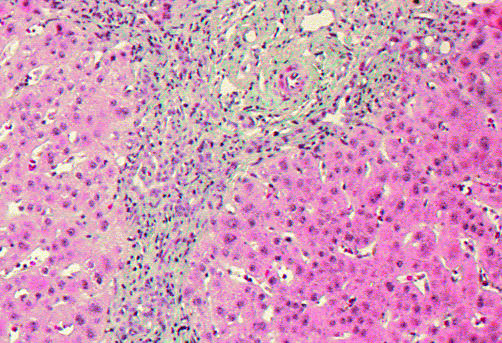
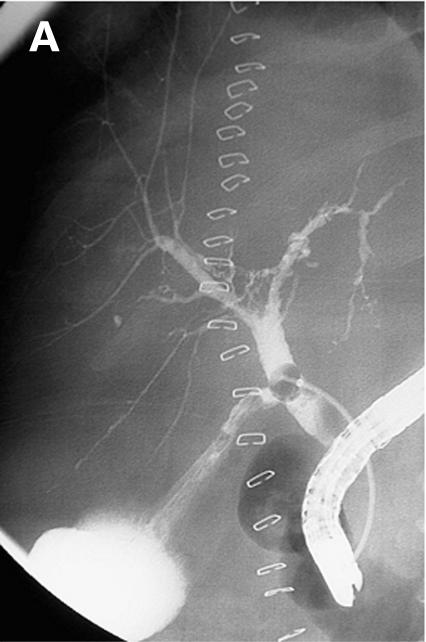
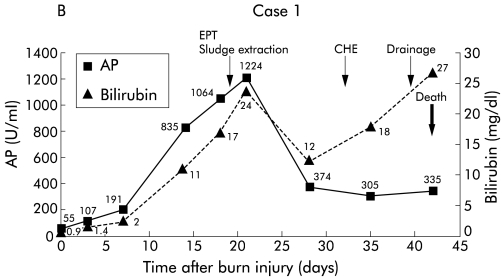
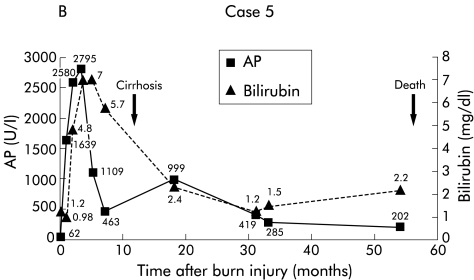
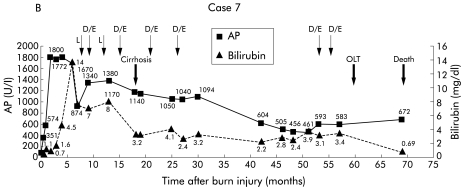
Patients: All nine patients had previously required long term treatment in an intensive care unit for septic shock: two patients with polytrauma, five with burn injury, and two with extensive surgery. They were admitted to our hospital because of cholangitis. Endoscopic retrograde cholangiography revealed severe intrahepatic stenoses in all patients and liver biopsies showed typical signs of sclerosing cholangitis. No patient had pre-existing liver disease.
Results: Mean follow up time was 35 months. In patients with major bile duct stenoses (3/9), 12 endoscopic dilations were performed in total. In one patient, concrements were extracted and intermittent stenting was necessary. To date, 4/9 patients have rapidly developed liver cirrhosis. During follow up, 5/9 patients died: two after fulminant cholangitis, one after liver failure, one due to liver transplantation associated problems, and one after cerebral ischaemia. One patient has been registered for transplantation and the remaining three patients show no acute signs of liver failure.
Conclusions: Patients with sclerosing cholangitis, following septic shock, represent a new variant of vanishing bile duct disorders. In such patients liver disease rapidly progresses to cirrhosis. Endoscopic treatment may only transiently improve the course of the disease. Orthotopic liver transplantation is indicated in end stage disease.
Figures


References
-
- Desmet VJ. Vanishing bile duct disorders. In: Boyer JL, Ockner RK, eds. Progress in Liver Diseases, vol X. Philadelphia: WB Saunders; 1992:89–121. - PubMed
-
- Desmet VJ, van Eyken P, Roskams T. Histopathology of vanishing bile duct diseases. Adv Clin Path 1998;2:87–99. - PubMed
-
- Amor A, Chapoutot C, Michel J, et al. Secondary sclerosing cholangitis. Presse Med 1995;24:948–52. - PubMed
-
- Loinaz C, Gonzalez EM, Jimenez C, et al. Long-term biliary complications after liver surgery leading to liver transplantation. World J Surg 2001;25:1260–3. - PubMed
-
- Schmitt M, Kölbel CB, Müller MK, et al. Sklerosierende Cholangitis nach Verbrennung. Z Gastroenterol 1997;35:929–34. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources