

Increases in free radicals and cytoskeletal protein oxidation and nitration in the colon of patients with inflammatory bowel disease
- PMID: 12692059
- PMCID: PMC1773652
- DOI: 10.1136/gut.52.5.720
Increases in free radicals and cytoskeletal protein oxidation and nitration in the colon of patients with inflammatory bowel disease
Abstract
Background: Overproduction of colonic oxidants contributes to mucosal injury in inflammatory bowel disease (IBD) but the mechanisms are unclear. Our recent findings using monolayers of intestinal cells suggest that the mechanism could be oxidant induced damage to cytoskeletal proteins. However, oxidants and oxidative damage have not been well characterised in IBD mucosa.
Aims: To determine whether there are increases in oxidants and in tissue and cytoskeletal protein oxidation in IBD mucosa.
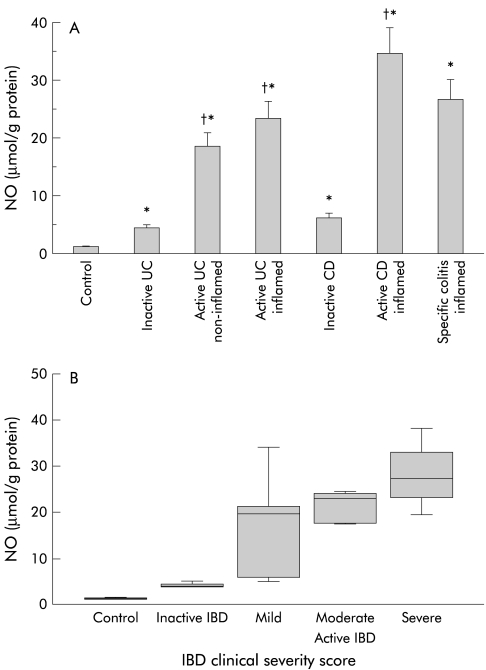
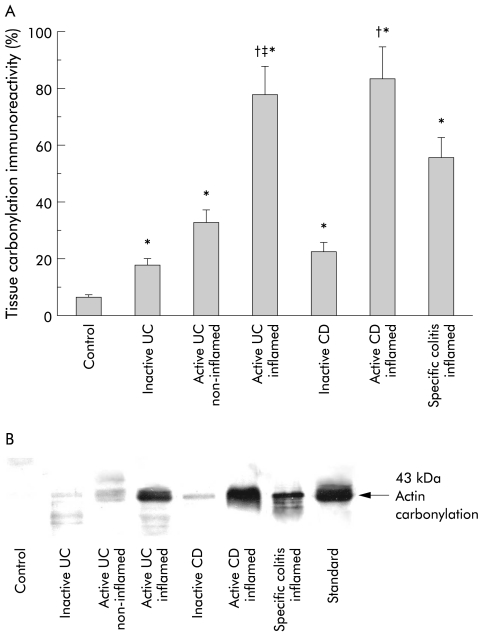
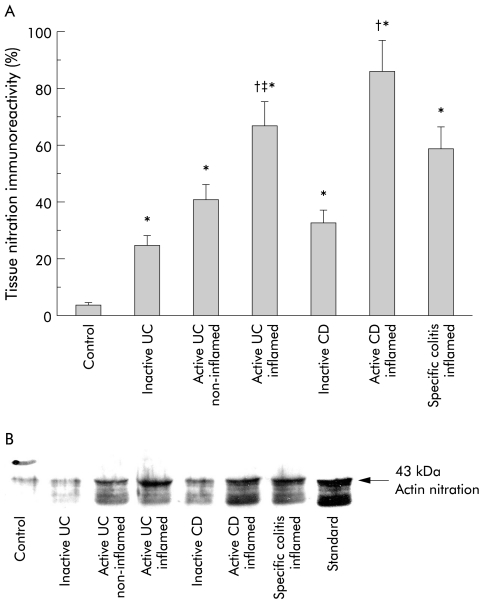
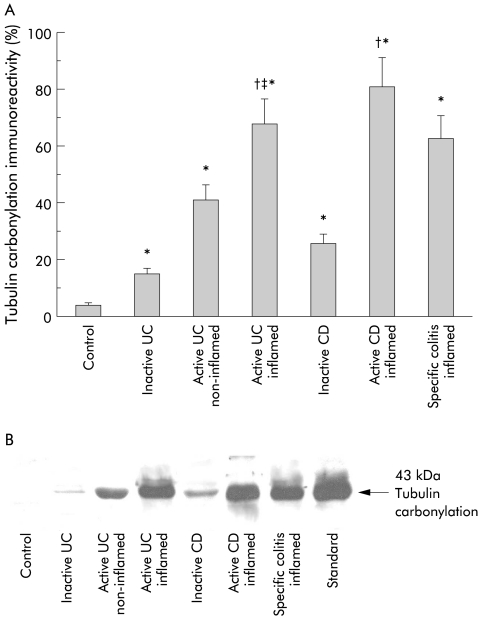
Methods: We measured nitric oxide (NO) and markers of oxidative injury (carbonylation and nitrotyrosination) to tissue and cytoskeletal proteins in colonic mucosa from IBD patients (ulcerative colitis, Crohn's disease, specific colitis) and controls. Outcomes were correlated with IBD severity score.
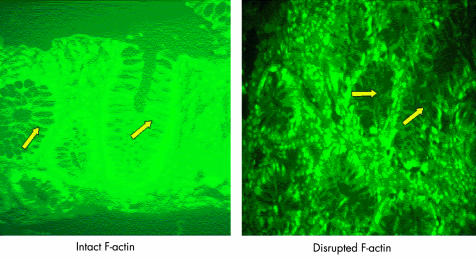
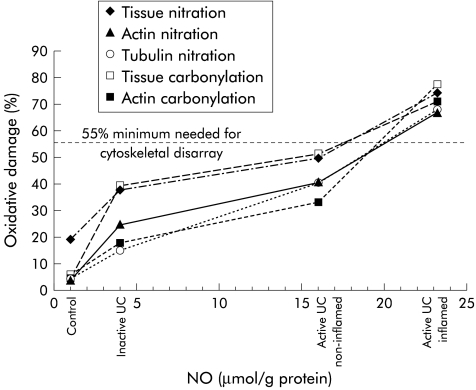
Results: Inflamed mucosa showed the greatest increases in oxidants and oxidative damage. Smaller but still significant increases were seen in normal appearing mucosa of patients with active and inactive IBD. Tissue NO levels correlated with oxidative damage. Actin was markedly (>50%) carbonylated and nitrated in inflamed tissues of active IBD, less so in normal appearing tissues. Tubulin carbonylation occurred in parallel; tubulin nitration was not observed. NO and all measures of oxidative damage in tissue and cytoskeletal proteins in the mucosa correlated with IBD severity. Disruption of the actin cytoarchitecture was primarily within the epithelial cells and paracellular area.
Conclusions: Oxidant levels increase in IBD along with oxidation of tissue and cytoskeletal proteins. Oxidative injury correlated with disease severity but is also present in substantial amounts in normal appearing mucosa of IBD patients, suggesting that oxidative injury does not necessarily lead to tissue injury and is not entirely a consequence of tissue injury. Marked actin oxidation (>50%)-which appears to result from cumulative oxidative damage-was only seen in inflamed mucosa, suggesting that oxidant induced cytoskeletal disruption is required for tissue injury, mucosal disruption, and IBD flare up.
Figures



References
-
- Simmonds NJ, Allen RE, Stevens TRJ, et al. Chemiluminescence assay of mucosal active oxygen metabolites in inflammatory bowel disease. Gastroenterology 1989;103:186–96. - PubMed
-
- Keshavarzian A, Sedghi S, Kanofsky J, et al. Excessive production of reactive oxygen metabolites by inflamed colon: Analysis by chemiluminescence probe. Gastroenterology 1992;103:177–85. - PubMed
-
- Harris ML, Schiller HJ, Reilly PM, et al. Free radicals and other reactive oxygen metabolites in inflammatory bowel disease: cause, consequence or epiphenomenon? Pharmacol Ther 1992;53:375–408. - PubMed
-
- Grisham MB, Yamada T. Neutrophils, nitrogen oxides and inflammatory bowel disease. Ann N Y Acad Sci 1992;664:103–15. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical