

Diffusion-tensor imaging for the detection and quantification of treatment-induced white matter injury in children with medulloblastoma: a pilot study
- PMID: 12695214
- PMCID: PMC8148675
Diffusion-tensor imaging for the detection and quantification of treatment-induced white matter injury in children with medulloblastoma: a pilot study
Abstract
Background and purpose: Treatment-induced white matter (WM) injury in medulloblastoma survivors, as manifested by deterioration of cognitive function, is prevalent. However, no reliable imaging method exists for early detection and quantification. Our goal was to determine whether anisotropy of WM is reduced in medulloblastoma survivors and whether fractional anisotropy (FA) can be used as an index for evaluation of treatment-induced WM injury.
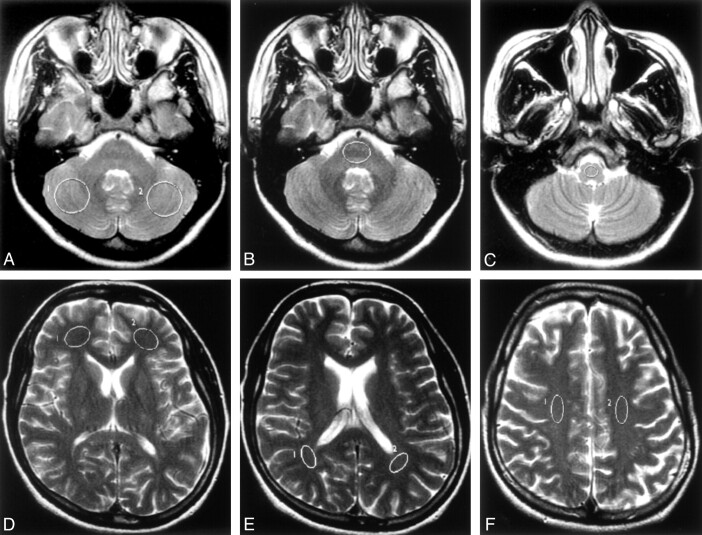
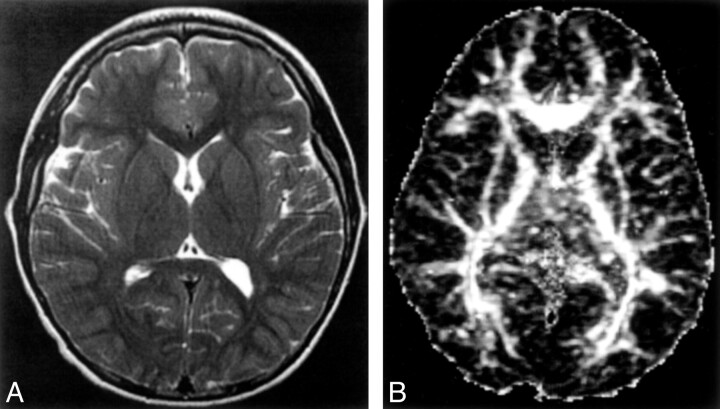
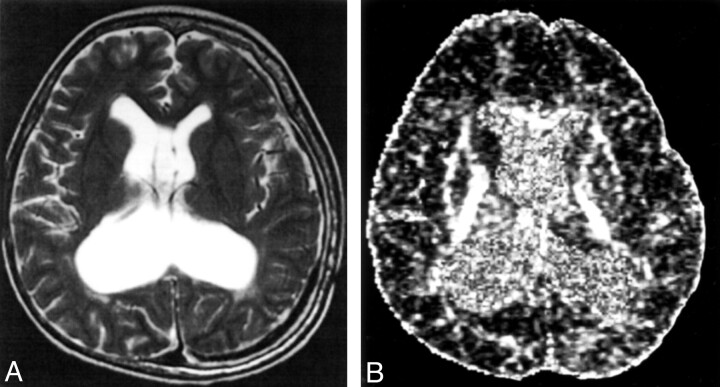
Methods: We evaluated nine medulloblastoma survivors treated with surgery, cranial irradiation, and chemotherapy by use of diffusion-tensor (DT) imaging and compared FA findings in selected WM sites (cerebellar hemispheres, pons, medulla oblongata, frontal periventricular WM, parietal periventricular WM, and corona radiata) with those of healthy age-matched control subjects. FA maps were compared with conventional T2-weighted images. FA was also compared with age at treatment, time interval since treatment, and deterioration of school performance. The two-tailed paired t test was used to determine statistical significance (P <.05).
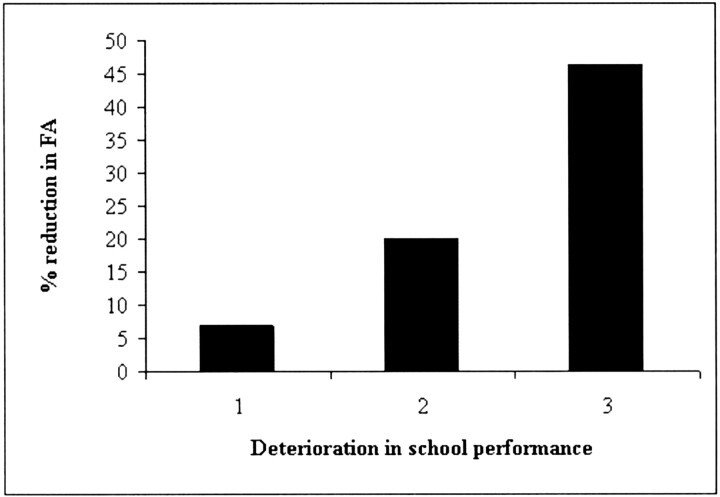
Results: Significant reduction of FA (P <.05) was seen in all anatomic sites in the patient group compared with FA in control subjects, except in the frontal periventricular WM, even in areas with normal appearance on T2-weighted images. FA reduction ranged from 12.4-19% (mean, 16.5%). Compared with control subjects, posterior fossa and supratentorial WM FA in patients were reduced by 14.6% (SD 1.9%) and 18.4% (SD 0.55%), respectively (P =.029). Reduction of supratentorial WM FA correlated with younger age at treatment (< 5 years), longer interval since treatment (> 5 years), and deterioration of school performance.
Conclusion: DT imaging and use of the index FA is potentially useful for early detection and monitoring of treatment-induced WM injury in children with medulloblastoma.
Figures
Similar articles
-
White-matter diffusion anisotropy after chemo-irradiation: a statistical parametric mapping study and histogram analysis.Neuroimage. 2004 Jan;21(1):261-8. doi: 10.1016/j.neuroimage.2003.09.020. Neuroimage. 2004. PMID: 14741664
-
Cerebral white matter fractional anisotropy and tract volume as measured by MR imaging are associated with impaired cognitive and motor function in pediatric posterior fossa tumor survivors.Pediatr Blood Cancer. 2015 Jul;62(7):1252-8. doi: 10.1002/pbc.25485. Epub 2015 Apr 7. Pediatr Blood Cancer. 2015. PMID: 25850573
-
Diffusion tensor magnetic resonance imaging finding of discrepant fractional anisotropy between the frontal and parietal lobes after whole-brain irradiation in childhood medulloblastoma survivors: reflection of regional white matter radiosensitivity?Int J Radiat Oncol Biol Phys. 2007 Nov 1;69(3):846-51. doi: 10.1016/j.ijrobp.2007.04.041. Epub 2007 Jun 4. Int J Radiat Oncol Biol Phys. 2007. PMID: 17544593
-
The role of diffusion tensor imaging and fractional anisotropy in the evaluation of patients with idiopathic normal pressure hydrocephalus: a literature review.Neurosurg Focus. 2016 Sep;41(3):E12. doi: 10.3171/2016.6.FOCUS16192. Neurosurg Focus. 2016. PMID: 27581308 Review.
-
Cognitive disorders in pediatric medulloblastoma: what neuroimaging has to offer.J Neurosurg Pediatr. 2014 Aug;14(2):136-44. doi: 10.3171/2014.5.PEDS13571. Epub 2014 Jun 20. J Neurosurg Pediatr. 2014. PMID: 24950472 Review.
Cited by
-
Evaluation of normal-appearing white matter with perfusion and diffusion MRI in patients with treated glioblastoma.MAGMA. 2022 Feb;35(1):153-162. doi: 10.1007/s10334-021-00990-5. Epub 2021 Dec 24. MAGMA. 2022. PMID: 34951690
-
Regional white matter anisotropy and reading ability in patients treated for pediatric embryonal tumors.Brain Imaging Behav. 2010 Jun;4(2):132-40. doi: 10.1007/s11682-010-9092-1. Brain Imaging Behav. 2010. PMID: 20502994 Free PMC article.
-
Neurodevelopmental impact on children treated for medulloblastoma: a review and proposed conceptual model.Dev Disabil Res Rev. 2008;14(3):203-10. doi: 10.1002/ddrr.32. Dev Disabil Res Rev. 2008. PMID: 18924159 Free PMC article. Review.
-
Differences in brainstem fiber tract response to radiation: a longitudinal diffusion tensor imaging study.Int J Radiat Oncol Biol Phys. 2013 Jun 1;86(2):292-7. doi: 10.1016/j.ijrobp.2013.01.028. Epub 2013 Mar 6. Int J Radiat Oncol Biol Phys. 2013. PMID: 23474114 Free PMC article.
-
Diffusion tensor imaging of deep gray matter in children treated for brain malignancies.Childs Nerv Syst. 2014 Apr;30(4):631-8. doi: 10.1007/s00381-013-2315-1. Epub 2013 Nov 22. Childs Nerv Syst. 2014. PMID: 24264381 Free PMC article.
References
-
- Packer RJ, Goldwein J, Nicholson HS, et al. Treatment of children with medulloblastomas with reduced-dose craniospinal radiation therapy and adjuvant chemotherapy: a Children’s Cancer Group Study. J Clin Oncol 1999;17:2127–2136 - PubMed
-
- Chan GCF, Li CK, Luk CW, et al. Treatment of childhood medulloblastoma with combined chemotherapy and craniospinal irradiation: the Hong Kong Experience. Neurooncology 2002. (abstract, in press)
-
- Johnson DL, McCabe MA, Nicholson HS, et al. Quality of long-term survival in young children with medulloblastoma. J Neurosurg 1994;80:1004–1010 - PubMed
-
- Walter AW, Mulhern RK, Gajjar A, et al. Survival and neurodevelopmental outcome of young children with medulloblastoma at St. Jude Children’s Research Hospital. J Clin Oncol 1999;17:3720–3728 - PubMed
-
- Packer RJ, Sposto R, Atkins TE, et al. Quality of life in children with primitive neuroectodermal tumors (medulloblastoma) of the posterior fossa. Pediatr Neurosci 1987;13:169–175 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources