

Surgical physiology of inguinal hernia repair--a study of 200 cases
- PMID: 12697071
- PMCID: PMC155644
- DOI: 10.1186/1471-2482-3-2
Surgical physiology of inguinal hernia repair--a study of 200 cases
Abstract
Background: Current inguinal hernia operations are generally based on anatomical considerations. Failures of such operations are due to lack of consideration of physiological aspects. Many patients with inguinal hernia are cured as a result of current techniques of operation, though factors that are said to prevent hernia formation are not restored. Therefore, the surgical physiology of inguinal canal needs to be reconsidered.
Methods: A retrospective study is describer of 200 patients operated on for inguinal hernia under local anaesthesia by the author's technique of inguinal hernia repair.
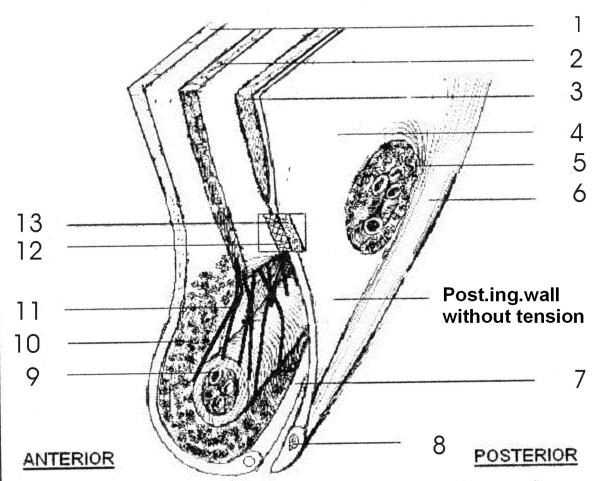
Results: The posterior wall of the inguinal canal was weak and without dynamic movement in all patients. Strong aponeurotic extensions were absent in the posterior wall. The muscle arch movement was lost or diminished in all patients. The movement of the muscle arch improved after it was sutured to the upper border of a strip of the external oblique aponeurosis (EOA). The newly formed posterior wall was kept physiologically dynamic by the additional muscle strength provided by external oblique muscle to the weakened muscles of the muscle arch.
Conclusions: A physiologically dynamic and strong posterior inguinal wall, and the shielding and compression action of the muscles and aponeuroses around the inguinal canal are important factors that prevent hernia formation or hernia recurrence after repair. In addition, the squeezing and plugging action of the cremasteric muscle and binding effect of the strong cremasteric fascia, also play an important role in the prevention of hernia.
Figures




References
-
- Lytle WJ. The internal inguinal ring. Br J Surg. 1945;32:441.
-
- Hammond TE. The etiology of indirect inguinal hernia. Lancet. 1923;204:1206. doi: 10.1016/S0140-6736(00)45516-9. - DOI
-
- Keith A. On the origin and nature of hernia. Br J Surg. 1923;11:455.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
