

Review
doi: 10.1056/NEJMcp021804.
Clinical practice. Mammographic screening for breast cancer
Affiliations
- PMID: 12711743
- PMCID: PMC3157308
- DOI: 10.1056/NEJMcp021804
Item in Clipboard
Review
Clinical practice. Mammographic screening for breast cancer
N Engl J Med.
.
Abstract
A 44-year-old woman who is a new patient has no known current health problems and no family history of breast or ovarian cancer. Eighteen months ago, she had a normal screening mammogram. She recently read that mammograms may not help to prevent death from breast cancer and that “the patient should decide.” But she does not think she knows enough. She worries that there is a breast-cancer epidemic. What should her physician advise?
Figures
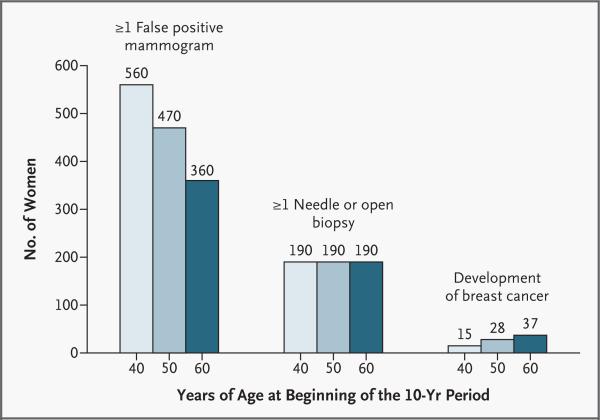
All numbers are rounded. The numbers for 10-year rates of false positive mammograms and breast biopsies come from a single study in which, overall, the rate of false positive mammograms was 6.5 percent, and the rate may be different in other settings. Data on the development of breast cancer are broken down further in Figure 2.
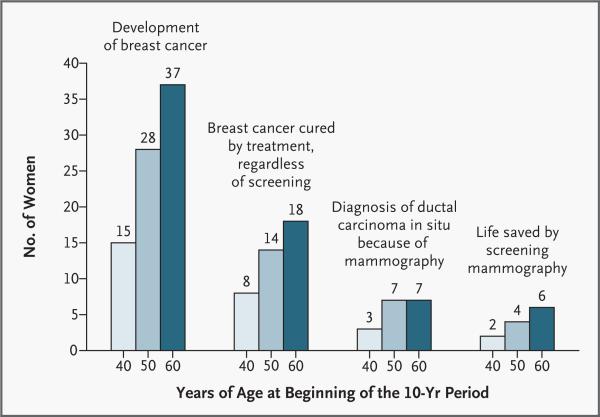
All numbers are rounded. The numbers for the incidence of invasive breast cancer and ductal carcinoma in situ, as well as the number of women whose lives are saved by treatment (those surviving at least 20 years after the first diagnosis of breast cancer) regardless of screening, were calculated on the basis of data from the Surveillance, Epidemiology, and End Results program., The numbers of women whose lives are saved because of screening (those surviving at least 15 years after diagnosis) were calculated on the assumption of a reduction of 20 percent in mortality from breast cancer among women 40 to 49 years of age and a reduction of 30 percent among women 50 to 69 years of age; these numbers are approximate.
Comment in
-
Mammographic screening for breast cancer.N Engl J Med. 2003 Aug 7;349(6):610-2; author reply 610-2. doi: 10.1056/NEJM200308073490617. N Engl J Med. 2003. PMID: 12904529 No abstract available.
-
Mammographic screening for breast cancer.N Engl J Med. 2003 Aug 7;349(6):610-2; author reply 610-2. N Engl J Med. 2003. PMID: 12908460 No abstract available.
-
Mammographic screening for breast cancer.N Engl J Med. 2003 Aug 7;349(6):610-2; author reply 610-2. N Engl J Med. 2003. PMID: 12908461 No abstract available.
-
Mammographic screening for breast cancer.N Engl J Med. 2003 Aug 7;349(6):610-2; author reply 610-2. N Engl J Med. 2003. PMID: 12908462 No abstract available.
-
Mammographic screening for breast cancer.N Engl J Med. 2003 Aug 7;349(6):610-2; author reply 610-2. N Engl J Med. 2003. PMID: 12908463 No abstract available.
References
-
- Ries LAG, Eisner MP, Kosary CL, et al., editors. SEER cancer statistics review, 1973-1999. National Cancer Institute; Bethesda, Md.: 2002. [April 1, 2003]. (at http://seer.cancer.gov/csr/1973_1999/.)
-
- Blackman DK, Bennett EM, Miller DS. Trends in self-reported use of mammograms (1989–1997) and Papanicolaou tests (1991–1997) —behavioral risk factor surveillance system. MMWR CDC Surveill Summ. 1999;48(SS-6):1–22. - PubMed
-
- Preventive Services Task Force Screening for breast cancer: recommendations and rationale. Ann Intern Med. 2002;137:344–6. - PubMed
-
- Johnson JD, Meishcke H. Differences in evaluations of communication channels for cancer-related information. J Behav Med. 1992;15:429–45. - PubMed
-
- Kinsinger L, Harris R, Karnitschnig J. Interest in decision-making about breast cancer screening in younger women. J Gen Intern Med. 1998;13(Suppl):98. abstract. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical