

Outcomes of screening to prevent cancer: analysis of cumulative incidence of cervical abnormality and modelling of cases and deaths prevented
- PMID: 12714468
- PMCID: PMC153831
- DOI: 10.1136/bmj.326.7395.901
Outcomes of screening to prevent cancer: analysis of cumulative incidence of cervical abnormality and modelling of cases and deaths prevented
Erratum in
- BMJ. 2003 Aug 9;327(7410):325
Abstract
Objective: To determine the frequency of different outcomes in women participating in cervical screening.
Design: Analysis of screening records from 348 419 women, and modelling of cases of cervical cancer and deaths with and without screening.
Setting: Cervical screening programme in Bristol.
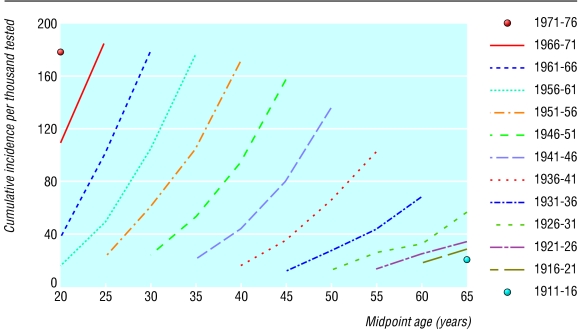
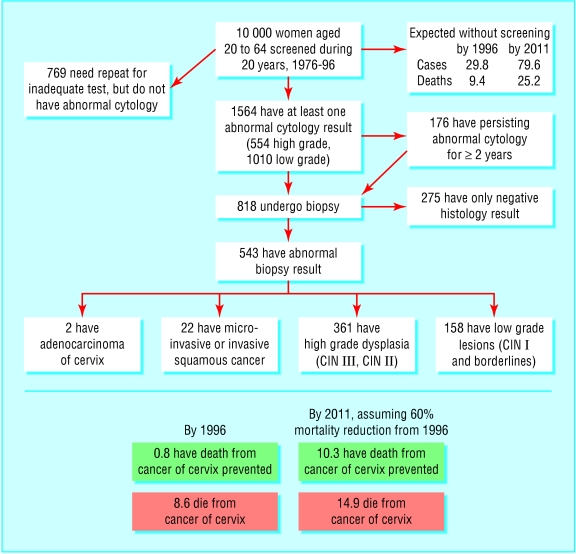
Results: For every 10 000 women screened from 1976 to 1996, 1564 had abnormal cytology, 818 were investigated, and 543 had abnormal histology. One hundred and seventy six had persistent abnormality for two years or more. In the absence of screening 80 women would be expected to develop cancer of the cervix by 2011, of whom 25 would die. With screening 10 of these deaths would be avoided. Comparison of cumulative abnormality rates with numbers expected to develop cancer in the absence of screening suggests that at least 80% of high grade dyskaryosis and of high grade dysplasia would not progress to cancer. The lifetime risk of having abnormal cytology detected could be as high as 40% for women born since 1960.
Conclusions: Screening is labour and resource intensive. It involves treatment for many women not destined to develop invasive cancer. The increased intervention rate for cervical abnormality in England is due to change in practice, not a cohort effect, and is probably the reason for the marked fall in incidence and mortality during the 1990s. For other cancers there is scope for major iatrogenic harm from screening because of invasive tests and treatments.
Figures
Comment in
-
Outcomes of screening to prevent cancer: think of screening as insurance.BMJ. 2003 Jul 5;327(7405):50; author reply 50. doi: 10.1136/bmj.327.7405.50. BMJ. 2003. PMID: 12842960 Free PMC article. No abstract available.
References
-
- Raffle AE, Alden B, Mackenzie EF. Detection rates for abnormal cervical smears: what are we screening for? Lancet. 1995;345:1469–1473. - PubMed
-
- Anderson CM, Nottingham J. Bridging the knowledge gap and communicating uncertainties for informed consent in cervical cytology screening: we need unbiased information and a culture change. Cytopathology. 1999;10:221–228. - PubMed