

Recurrent cecocolic torsion: radiological diagnosis and treatment
- PMID: 12722995
- PMCID: PMC3015465
Recurrent cecocolic torsion: radiological diagnosis and treatment
Abstract
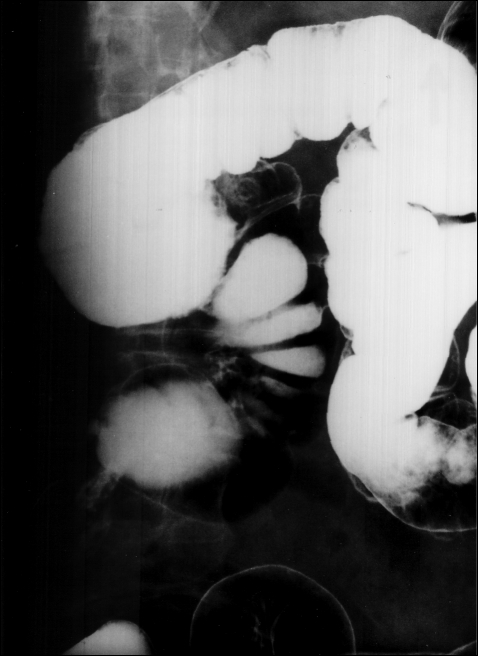
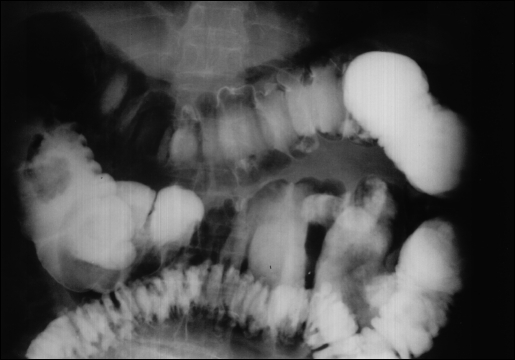
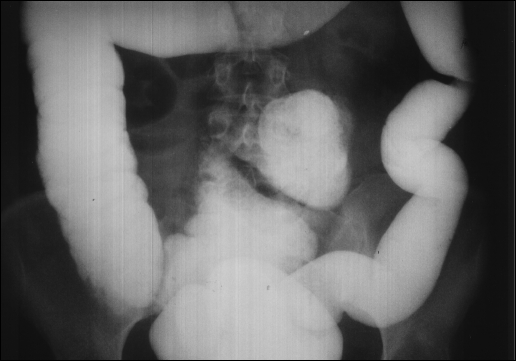
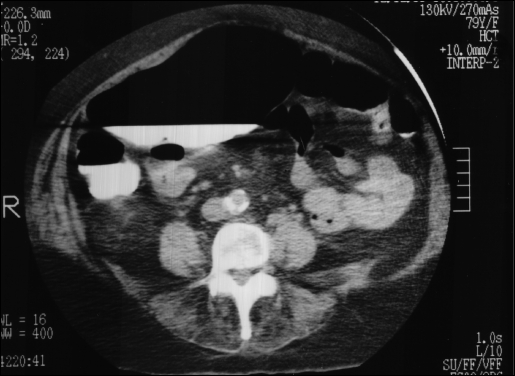
Recurrent cecocolic torsion may cause recurrent right lower abdominal pain and right-sided thrust dyspareunia. It is seldom considered in the differential diagnosis of pain in this region. The propensity of the cecocolon to torse is secondary to the double developmental defect of a mobile cecocolon compounded by an elongated and overrotated organ that can be eccentrically located in the abdomen. The torsion may result in recurrent obstructions with spontaneous resolutions, but it may proceed to an acute episode of obstruction and strangulation with a more profound morbidity and mortality rate. The diagnosis of recurrent cecocolic torsion is verified by a plain x-ray film of the abdomen, contrast enema, and computed tomography scan. The preferred treatment is outpatient laparoscopic cecocolopexy. Laparoscopic or classical open cecocolectomy and right hemicolectomy are reserved for more complex and morbid presentations.
Figures






Similar articles
-
Cecocolic torsion: classification, pathogenesis, and treatment.JSLS. 2005 Jul-Sep;9(3):328-34. JSLS. 2005. PMID: 16121881 Free PMC article.
-
[Colon CT exploration of an internal hernia of the ascending cecocolon through the hiatus of Winslow].J Radiol. 2007 Mar;88(3 Pt 1):393-6. doi: 10.1016/s0221-0363(07)89837-4. J Radiol. 2007. PMID: 17457272 French. No abstract available.
-
[Cecal herniation through the foramen of Winslow as a rare cause of ileus].Rozhl Chir. 2016 Summer;95(7):291-3. Rozhl Chir. 2016. PMID: 27523178 Czech.
-
[Cecal volvulus].J Chir (Paris). 2005 Jul-Aug;142(4):220-4. doi: 10.1016/s0021-7697(05)80907-x. J Chir (Paris). 2005. PMID: 16335894 Review. French.
-
Torsion of vermiform appendix: value of ultrasonographic findings.Eur J Pediatr Surg. 1998 Dec;8(6):376-7. doi: 10.1055/s-2008-1071238. Eur J Pediatr Surg. 1998. PMID: 9926311 Review.
Cited by
-
Caecal volvulus on a background of recurrent caecocolic torsion.Ann R Coll Surg Engl. 2021 May;103(5):e177-e179. doi: 10.1308/rcsann.2020.7114. Epub 2021 Mar 8. Ann R Coll Surg Engl. 2021. PMID: 33682464 Free PMC article.
-
Multimodality imaging of cecal bascule: report of a case following pelvic surgery.Clin J Gastroenterol. 2012 Jun;5(3):225-9. doi: 10.1007/s12328-012-0306-5. Epub 2012 May 9. Clin J Gastroenterol. 2012. PMID: 26182325
-
Laparoscopic Management of Mobile Cecum.JSLS. 2016 Oct-Dec;20(4):e2016.00076. doi: 10.4293/JSLS.2016.00076. JSLS. 2016. PMID: 27807396 Free PMC article.
-
Cecocolic torsion: classification, pathogenesis, and treatment.JSLS. 2005 Jul-Sep;9(3):328-34. JSLS. 2005. PMID: 16121881 Free PMC article.
References
-
- Tirol FT. Dyspareunia: A symptom of cecocolic torsion. Abdm Surg. Fall 2001;11–15
-
- Anderson JR, Welch GH. Acute volvulus of the right colon; an analysis of 69 patients. World J Surg. 1986;10:336–342 - PubMed
-
- Rabinovici R, Simansky DA, Kaplan O, Mavor E, Manny J. Cecal Volvulus. Dis Colon Rectum. 1990;33:765–769. - PubMed
-
- Wolf BG. Volvulus of the colon. In: Cameron JL. ed, Current Surgical Therapy. 3rd ed Toronto, Canada: BC Decker Inc; 1989:130–131
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical