

Sestamibi scanning and minimally invasive radioguided parathyroidectomy without intraoperative parathyroid hormone measurement
- PMID: 12724639
- PMCID: PMC1514518
- DOI: 10.1097/01.SLA.0000064362.58751.59
Sestamibi scanning and minimally invasive radioguided parathyroidectomy without intraoperative parathyroid hormone measurement
Abstract
Objective: To evaluate the results of a large series of patients undergoing minimally invasive radioguided parathyroidectomy (MIRP) in which routine use of the intraoperative parathyroid hormone assay was not used, and to investigate characteristics between patients who had positive preoperative parathyroid scans versus those with negative scans.
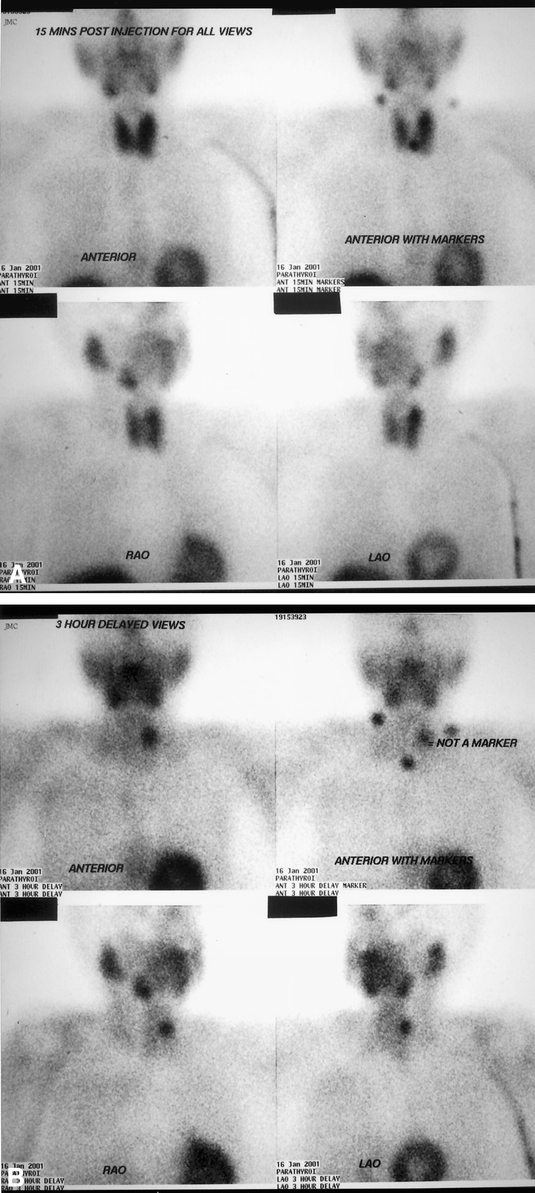
Summary background data: The technique of parathyroidectomy has traditionally involved bilateral exploration of the neck under general endotracheal anesthesia. Parathyroid imaging using technetium-99m sestamibi (MIBI) has evolved and can localize the adenomas in 80% to 90% of patients. The MIRP technique combines parathyroid scintigraphy with a hand-held gamma detector used intraoperatively to guide the surgeon to the adenoma in patients with positive MIBI scans. Central to this technique or other unilateral approaches is a positive MIBI scan.
Methods: One hundred seventy-three patients with primary hyperparathyroidism operated on by a single surgeon between January 1998 and July 2002 were included. One hundred twelve patients underwent the MIRP procedure and by definition had a positive preoperative parathyroid scan. The technique involved injecting 20 mCi MIBI 1 hour before the surgical procedure in patients who preoperatively had positive MIBI imaging. Patients had the choice of general or MAC anesthesia. Using an incision of less than 4 cm, the dissection to the adenoma was guided by the Navigator 11-mm probe. These 112 patients and 4 additional patients who for various reasons did not have the MIRP procedure yet had positive MIBI scans were compared to 57 patients who had clearly negative MIBI parathyroid imaging.
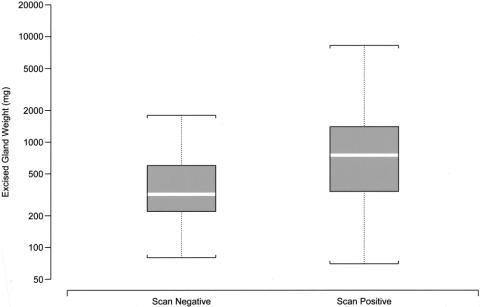
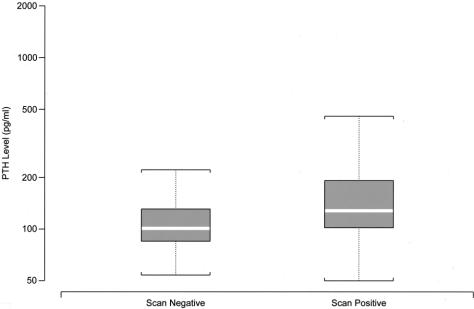
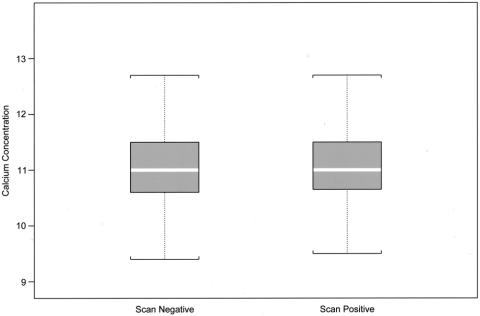
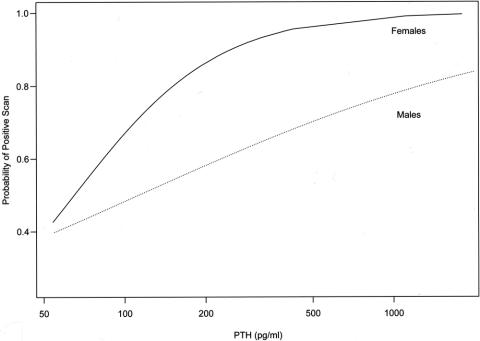
Results: Follow-up data were available for 108 of 112 patients who underwent MIRP. No patients had persistent hypercalcemia. The long-term success rate for the MIRP group was 98%. Fifty-two percent of the MIRP procedures were performed using MAC anesthesia. Overall, gland weight and serum PTH were related to the probability of a positive MIBI scan. Multiple logistic regression revealed that females were more likely to exhibit positive scans than were males for any fixed serum PTH level. For females, there was a significant relationship between increasing serum parathyroid hormone and a positive MIBI scan. Conversely, in males, the relationship between scan positivity and serum parathyroid hormone was weaker.
Conclusions: The MIRP technique without routine intraoperative serum parathyroid hormone measurement resulted in an excellent cure rate for primary hyperparathyroidism. As the MIRP technique as well as other techniques for unilateral cervical exploration are predicated on a positive parathyroid scan, the possible effect of gender on the sensitivity of MIBI scintigraphy for the detection of parathyroid adenomas warrants further investigation.
Figures
Similar articles
-
Effect of minimally invasive radioguided parathyroidectomy on efficacy, length of stay, and costs in the management of primary hyperparathyroidism.Ann Surg. 2000 May;231(5):732-42. doi: 10.1097/00000658-200005000-00014. Ann Surg. 2000. PMID: 10767795 Free PMC article.
-
Feasibility and safety of minimally invasive radioguided parathyroidectomy using very low intraoperative dose of Tc-99m MIBI.Int J Surg. 2017 Mar;39:229-233. doi: 10.1016/j.ijsu.2017.02.009. Epub 2017 Feb 10. Int J Surg. 2017. PMID: 28192245
-
Clinical role of 99mTcO4/MIBI scan, ultrasound and intra-operative gamma probe in the performance of unilateral and minimally invasive surgery in primary hyperparathyroidism.Eur J Nucl Med. 2001 Sep;28(9):1351-9. Eur J Nucl Med. 2001. PMID: 11585294
-
Minimally invasive radioguided parathyroidectomy (MIRP).Minerva Chir. 2003 Jun;58(3):269-79. Minerva Chir. 2003. PMID: 12955045 Review.
-
Preoperative localization and radioguided parathyroid surgery.J Nucl Med. 2003 Sep;44(9):1443-58. J Nucl Med. 2003. PMID: 12960191 Review.
Cited by
-
Could the eZ-SCOPE AN gamma camera replace intraoperative measurement of iPTH for PHPT?Int Surg. 2012 Apr-Jun;97(2):99-103. doi: 10.9738/CC138.1. Int Surg. 2012. PMID: 23102074 Free PMC article. Clinical Trial.
-
Minimally invasive parathyroidectomy with operative ultrasound localization of the adenoma.Surg Endosc. 2004 Jul;18(7):1097-8. doi: 10.1007/s00464-003-9228-0. Epub 2004 May 12. Surg Endosc. 2004. PMID: 15136931
-
The Relationship between Planar and SPECT/CT Parameters and Functional Markers in Primary Hyperparathyroidism.Diagnostics (Basel). 2023 Oct 11;13(20):3182. doi: 10.3390/diagnostics13203182. Diagnostics (Basel). 2023. PMID: 37892003 Free PMC article.
-
Evaluation of switch from satellite laboratory to central laboratory for testing of intraoperative parathyroid hormone.Pract Lab Med. 2020 Aug 20;22:e00176. doi: 10.1016/j.plabm.2020.e00176. eCollection 2020 Nov. Pract Lab Med. 2020. PMID: 32923573 Free PMC article.
-
Fluorescence-guided minimally invasive parathyroidectomy: clinical experience with a novel intraoperative detection technique for parathyroid glands.World J Surg. 2010 Sep;34(9):2217-22. doi: 10.1007/s00268-010-0621-2. World J Surg. 2010. PMID: 20512496
References
-
- Palmer M, Jakobsson S, Akerstrom G, et al. Prevalence of hypercalcemia in a a health survery: a 14-year follow-up study of serum calcium values. Eur J Clin Invest. 1998; 18: 39–46. - PubMed
-
- Auguste LJ, Attie JN, Schnaap D. Initial failure of surgical exploration in patients with primary hyperparathyroidism. Am J Surg. 1990; 160: 333–336. - PubMed
-
- van Heerden JA, Grant CS. Surgical treatment of primary hyperparathyroidism: an institutional perspective. World J Surg. 1991; 15: 688–692. - PubMed
-
- Denham D, Norman J. Cost-effectiveness of preoperative sestamibi scan for primary hyperparathyroidism is dependent solely upon the surgeon’s choice of operative procedure. J Am Coll Surg. 1998; 186: 293–305. - PubMed
-
- Norman J, Chheda H. Minimally invasive parathyroidectomy facilitated by intraoperative nuclear mapping. Surgery. 1997; 122: 998–1004. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
