

Cost effectiveness of ward based non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease: economic analysis of randomised controlled trial
- PMID: 12727767
- PMCID: PMC153850
- DOI: 10.1136/bmj.326.7396.956
Cost effectiveness of ward based non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease: economic analysis of randomised controlled trial
Abstract
Objective: To evaluate the cost effectiveness of standard treatment with and without the addition of ward based non-invasive ventilation in patients admitted to hospital with an acute exacerbation of chronic obstructive pulmonary disease.
Design: Incremental cost effectiveness analysis of a randomised controlled trial.
Setting: Medical wards in 14 hospitals in the United Kingdom.
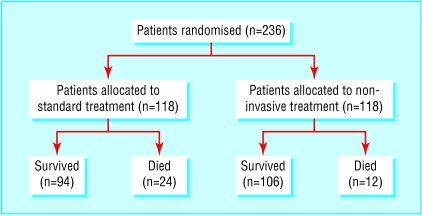
Participants: The trial comprised 236 patients admitted to hospital with an acute exacerbation of chronic obstructive pulmonary disease and mild to moderate acidosis (pH 7.25-7.35) secondary to respiratory failure. The economic analysis compared the costs of treatment that these patients received after randomisation.
Main outcome measure: Incremental cost per in-hospital death.
Results: 24/118 died in the group receiving standard treatment and 12/118 in the group receiving non-invasive ventilation (P=0.05). Allocation to the group receiving non-invasive ventilation was associated with a reduction in costs of 49362 pounds sterling (78741 dollars; 73109 euros), mainly through reduced use of intensive care units. The incremental cost effectiveness ratio was -645 pounds sterling per death avoided (95% confidence interval -2310 pounds sterling to 386 pounds sterling), indicating a dominant (more effective and less costly) strategy. Modelling of these data indicates that a typical UK hospital providing a non-invasive ventilation service will avoid six deaths and three to nine admissions to intensive care units per year, with an associated cost reduction of 12000-53000 pounds sterling per year.
Conclusions: Non-invasive ventilation is a highly cost effective treatment that both reduced total costs and improved mortality in hospital.
Figures
Comment in
-
Noninvasive ventilation was cost-effective for reducing in-hospital mortality in COPD.ACP J Club. 2004 Jan-Feb;140(1):23. ACP J Club. 2004. PMID: 14711294 No abstract available.
References
-
- Brochard L, Mancebo J, Wysocki M, Lofaso F, Conti G, Rauss A, et al. Non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 1995;333:817–822. - PubMed
-
- Kramer N, Meyer TJ, Meharg J, Cece RD, Hill NS. Randomised, prospective trial of noninvasive positive pressure ventilation in acute respiratory failure. Am J Respir Crit Care Med. 1995;151:1799–1806. - PubMed
-
- Martin TJ, Hovis JD, Costantino JP, Bierman MI, Donahue MP, Rogers RM, et al. A randomised prospective evaluation of non-invasive ventilation for acute respiratory failure. Am J Respir Crit Care Med. 2000;161:807–813. - PubMed
-
- Celikel T, Sungur M, Ceyhan B, Karakurt S. Comparison of non-invasive positive pressure ventilation with standard medical therapy in hypercapnic acute respiratory failure. Chest. 1998;114:1636–1642. - PubMed
-
- Plant PK, Owen JL, Elliott MW. Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial. Lancet. 2000;355:1931–1935. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical