

Explaining the de-prioritization of primary prevention: physicians' perceptions of their role in the delivery of primary care
- PMID: 12729463
- PMCID: PMC155789
- DOI: 10.1186/1471-2458-3-15
Explaining the de-prioritization of primary prevention: physicians' perceptions of their role in the delivery of primary care
Abstract
Background: While physicians are key to primary preventive care, their delivery rate is sub-optimal. Assessment of physician beliefs is integral to understanding current behavior and the conceptualization of strategies to increase delivery.
Methods: A focus group with regional primary care physician (PCP) Opinion Leaders was conducted as a formative step towards regional assessment of attitudes and barriers regarding preventive care delivery in primary care. Following the PRECEDE-PROCEED model, the focus group aim was to identify conceptual themes that characterize PCP beliefs and practices regarding preventive care. Seven male and five female PCPs (family medicine, internal medicine) participated in the audiotaped discussion of their perceptions and behaviors in delivery of primary preventive care. The transcribed audiotape was qualitatively analyzed using grounded theory methodology.
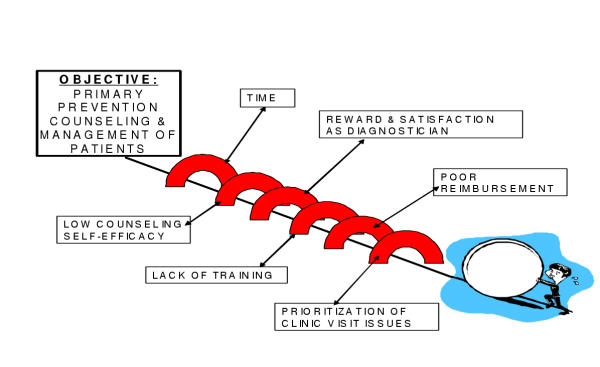
Results: The PCPs' own perceived role in daily practice was a significant barrier to primary preventive care. The prevailing PCP model was the "one-stop-shop" physician who could provide anything from primary to tertiary care, but whose provision was dominated by the delivery of immediate diagnoses and treatments, namely secondary care.
Conclusions: The secondary-tertiary prevention PCP model sustained the expectation of immediacy of corrective action, cure, and satisfaction sought by patients and physicians alike, and, thereby, de-prioritized primary prevention in practice. Multiple barriers beyond the immediate control of PCP must be surmounted for the full integration of primary prevention in primary care practice. However, independent of other barriers, physician cognitive value of primary prevention in practice, a base mediator of physician behavior, will need to be increased to frame the likelihood of such integration.
Figures
References
-
- Book Public Health Service Healthy People 2000: National Health Promotion and Disease Prevention Objectives. U.S. Department of Health and Human Services; 1990. Public Health Service. Healthy People 2000: National Health Promotion and Disease Prevention Objectives.
-
- Book Healthy People 2010. U.S. Department of Health and Human Services; 2000. Healthy People 2010. - PubMed
-
- Grol R, Grimshaw J. Evidence-based implementation of evidence-based medicine. Jt Comm J Qual Improv. 1999;25:503–513. - PubMed
-
- Hahn DL, Berger MG. Implementation of a systematic health maintenance protocol in a private practice. J Fam Pract. 1990;31:492–502; discussion 502-4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
