

Tolerogenic immunosuppression for organ transplantation
- PMID: 12737859
- PMCID: PMC2999636
- DOI: 10.1016/s0140-6736(03)13175-3
Tolerogenic immunosuppression for organ transplantation
Abstract
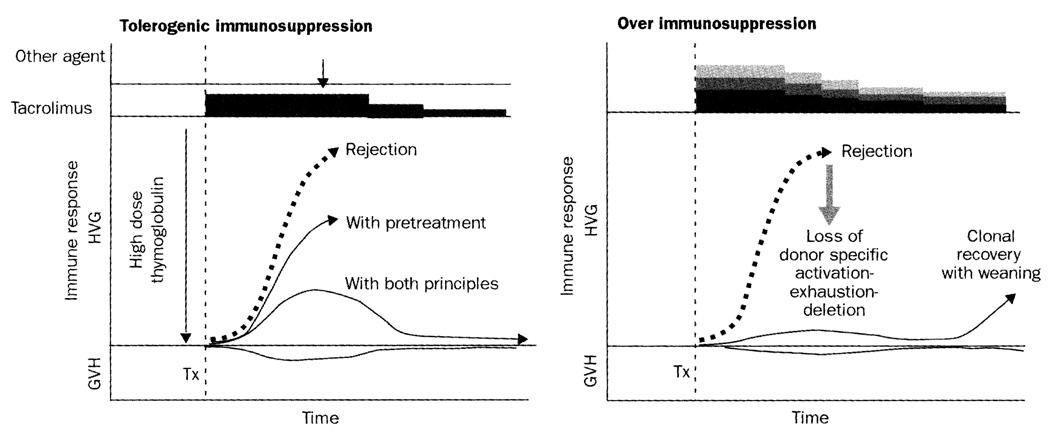
Background: Insight into the mechanisms of organ engraftment and acquired tolerance has made it possible to facilitate these mechanisms, by tailoring the timing and dosage of immunosuppression in accordance with two therapeutic principles: recipient pretreatment, and minimum use of post-transplant immunosuppression. We aimed to apply these principles in recipients of renal and extrarenal organ transplants.
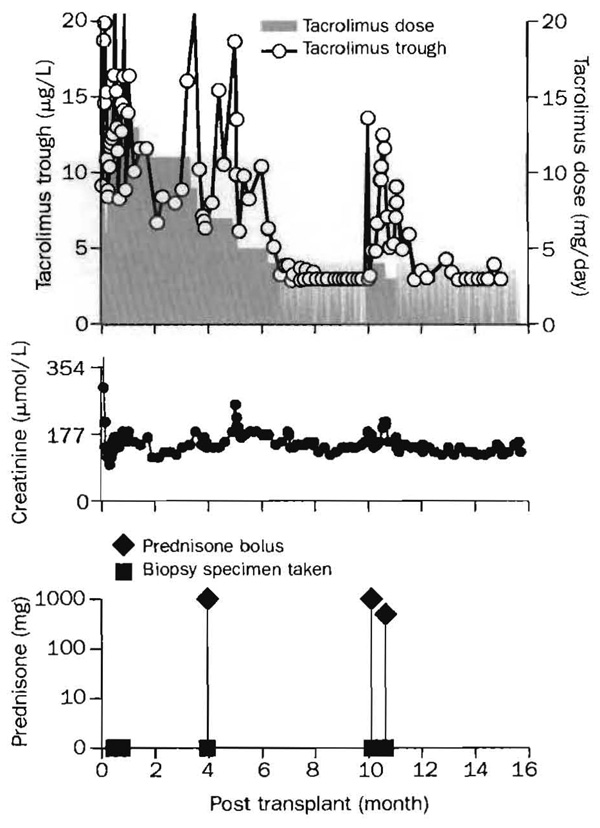
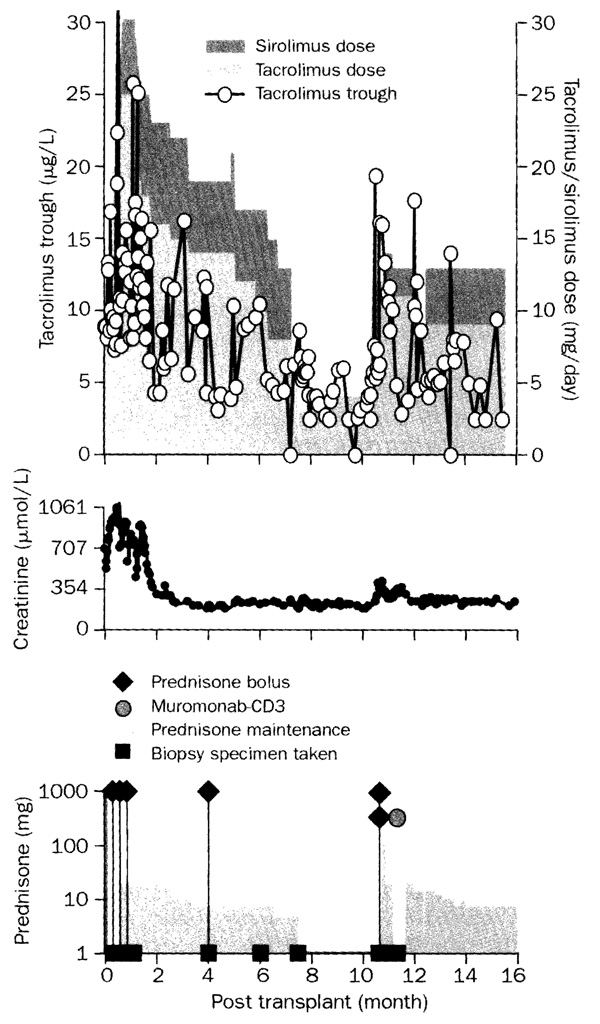
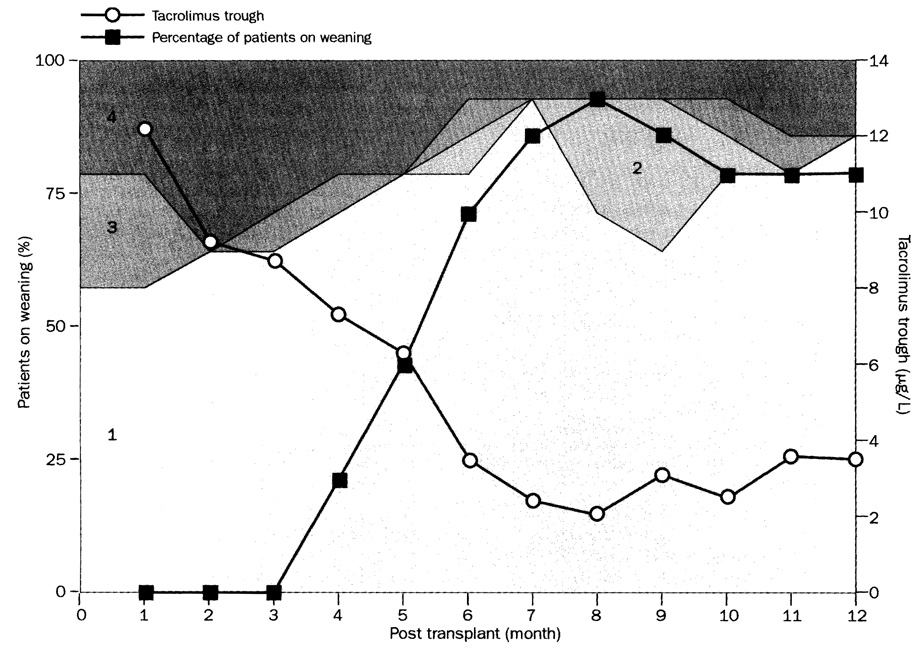
Methods: 82 patients awaiting kidney, liver, pancreas, or intestinal transplantation were pretreated with about 5 mg/kg of a broadly reacting rabbit antithymocyte globulin during several hours. Post-transplant immunosuppression was restricted to tacrolimus unless additional drugs were needed to treat breakthrough rejection. After 4 months, patients on tacrolimus monotherapy were considered for dose-spacing to every other day or longer intervals.
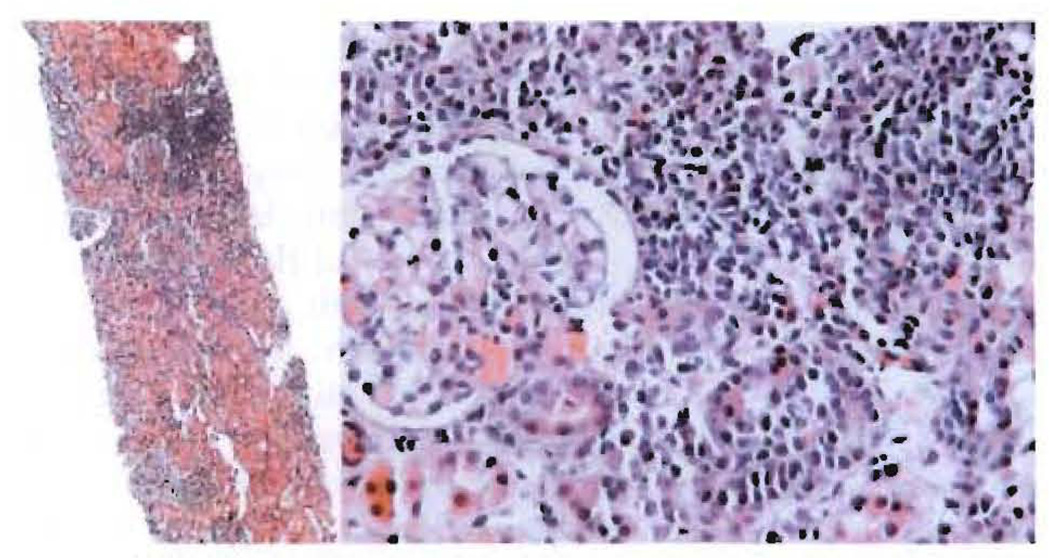
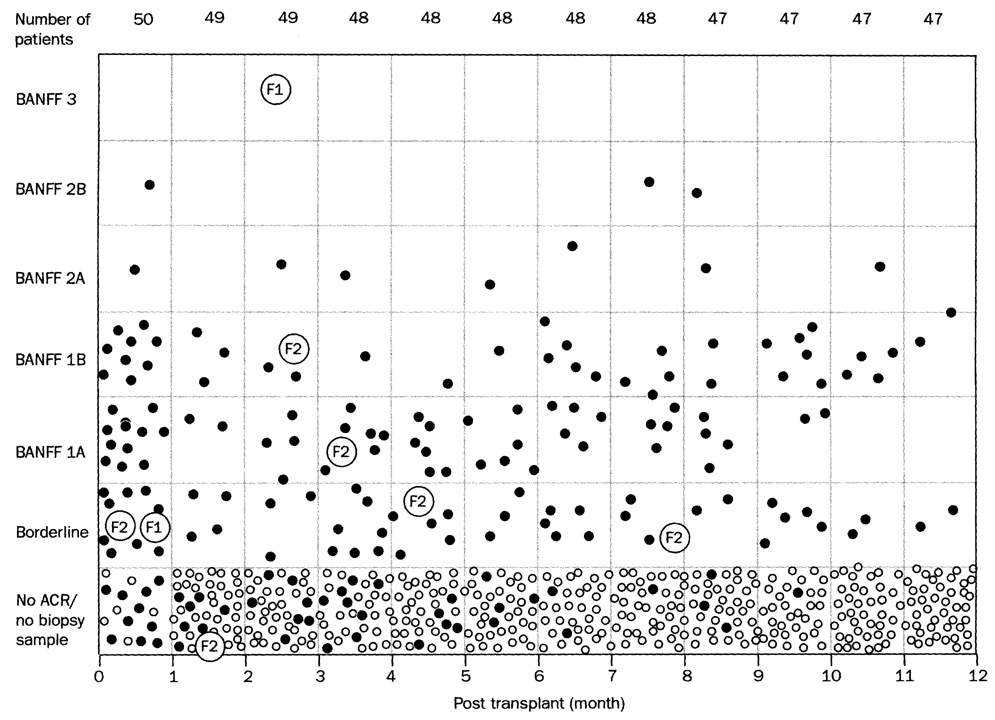
Findings: We frequently saw evidence of immune activation in graft biopsy samples, but unless this was associated with graft dysfunction or serious immune destruction, treatment usually was not intensified. Immunosuppression-related morbidity was virtually eliminated. 78 (95%) of 82 patients survived at 1 year and at 13-18 months. Graft survival was 73 (89%) of 82 at 1 year and 72 (88%) of 82 at 13-18 months. Of the 72 recipients with surviving grafts, 43 are on spaced doses of tacrolimus monotherapy: every other day (n=6), three times per week (11), twice per week (15), or once per week (11).
Interpretation: The striking ability to wean immunosuppression in these recipients indicates variable induction of tolerance. The simple therapeutic principles are neither drug-specific nor organ-specific. Systematic application of these principles should allow improvements in quality of life and long-term survival after organ transplantation.
Conflict of interest statement
Conflict of interest statement
None declared.
Figures


Comment in
-
Towards clinical transplantation tolerance.Lancet. 2003 May 3;361(9368):1489-90. doi: 10.1016/S0140-6736(03)13220-5. Lancet. 2003. PMID: 12737855 No abstract available.
-
Tolerance for immunosuppression in organ transplantation.Liver Transpl. 2004 Apr;10(4):573-5. doi: 10.1002/lt.20135. Liver Transpl. 2004. PMID: 15048805 No abstract available.
References
-
- Raeusen LC, Solez K, Colvin RB, et al. The Banff 97 working classification of renal allograft pathology. Kidney Int. 1999;55:713–723. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
