

The relationship between transplacental O2 diffusion and placental expression of PlGF, VEGF and their receptors in a placental insufficiency model of fetal growth restriction
- PMID: 12740423
- PMCID: PMC2343042
- DOI: 10.1113/jphysiol.2003.039511
The relationship between transplacental O2 diffusion and placental expression of PlGF, VEGF and their receptors in a placental insufficiency model of fetal growth restriction
Abstract
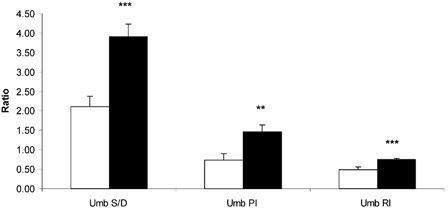
Placental growth factor (PlGF) and vascular endothelial growth factor (VEGF) are involved in placental angiogenesis through interactions with the VEGFR-1 and VEGFR-2 receptors. The placenta of pregnancies whose outcome is fetal growth restriction (FGR) are characterized by abnormal angiogenic development, classically associated with hypoxia. The present study evaluated the near-term expression of this growth factor family in an ovine model of placental insufficiency-FGR, in relationship to uteroplacental oxygenation. Compared to controls, FGR pregnancies demonstrated a 37% increase in uterine blood flow (FGR vs. control, 610.86+/-48.48 vs. 443.17+/-37.39 ml min(-1) (kg fetus)(-1); P<0.04), which was associated with an increased maternal uterine venous PO2 (58.13+/-1.00 vs. 52.89+/-1.26 mmHg; P<0.02), increased umbilical artery systolic/diastolic ratio (3.90+/-0.33 vs. 2.12+/-0.26, P<0.05), and fetal hypoxia (arterial PO2; 12.79+/-0.97 vs. 18.65+/-1.6 mmHg, P<0.005). Maternal caruncle PlGF mRNA was increased in FGR (P<0.02), while fetal cotyledon VEGF mRNA was reduced (P<0.02). VEGFR-1 mRNA was also reduced in FGR fetal cotyledon (P<0.001) but was not altered in caruncle tissue. Immunoblot analysis of PlGF and VEGF demonstrated single bands at 19,000 and 18,600 Mr, respectively. Caruncle PlGF concentration was increased (P<0.04), while cotyledon VEGF was decreased (P<0.05) in FGR placentae. The data establish that uterine blood flow is not reduced in relationship to metabolic demands in this FGR model and that the transplacental PO2 gradient is increased, maintaining umbilical oxygen uptake per unit of tissue. Furthermore, these data suggest that an increased transplacental gradient of oxygen generates changes in angiogenic growth factors, which may underline the pathophysiology of the post-placental hypoxic FGR.
Figures







Similar articles
-
Placental expression of VEGF, PlGF and their receptors in a model of placental insufficiency-intrauterine growth restriction (PI-IUGR).Placenta. 2002 Feb-Mar;23(2-3):132-44. doi: 10.1053/plac.2001.0757. Placenta. 2002. PMID: 11945079
-
Hypoxia down-regulates placenta growth factor, whereas fetal growth restriction up-regulates placenta growth factor expression: molecular evidence for "placental hyperoxia" in intrauterine growth restriction.Lab Invest. 1999 Feb;79(2):151-70. Lab Invest. 1999. PMID: 10068204
-
Fetal growth restriction: pathogenic mechanisms.Clin Obstet Gynecol. 2006 Jun;49(2):219-27. doi: 10.1097/00003081-200606000-00005. Clin Obstet Gynecol. 2006. PMID: 16721102 Review.
-
Down-regulation of placental neuropilin-1 in fetal growth restriction.Am J Obstet Gynecol. 2016 Feb;214(2):279.e1-279.e9. doi: 10.1016/j.ajog.2015.09.068. Epub 2015 Sep 26. Am J Obstet Gynecol. 2016. PMID: 26409917
-
Regulation of placental vascular endothelial growth factor (VEGF) and placenta growth factor (PIGF) and soluble Flt-1 by oxygen--a review.Placenta. 2000 Mar-Apr;21 Suppl A:S16-24. doi: 10.1053/plac.1999.0524. Placenta. 2000. PMID: 10831117 Review.
Cited by
-
Going Up Inflame: Reviewing the Underexplored Role of Inflammatory Programming in Stress-Induced Intrauterine Growth Restricted Livestock.Front Anim Sci. 2021 Nov;2:761421. doi: 10.3389/fanim.2021.761421. Epub 2021 Nov 4. Front Anim Sci. 2021. PMID: 34825243 Free PMC article.
-
ASAS-SSR Triennnial Reproduction Symposium: Looking Back and Moving Forward-How Reproductive Physiology has Evolved: Fetal origins of impaired muscle growth and metabolic dysfunction: Lessons from the heat-stressed pregnant ewe.J Anim Sci. 2018 Jun 29;96(7):2987-3002. doi: 10.1093/jas/sky164. J Anim Sci. 2018. PMID: 29701769 Free PMC article. Review.
-
Impact of chorionic somatomammotropin RNA interference on uterine blood flow and placental glucose uptake in the absence of intrauterine growth restriction.Am J Physiol Regul Integr Comp Physiol. 2021 Feb 1;320(2):R138-R148. doi: 10.1152/ajpregu.00223.2020. Epub 2020 Nov 4. Am J Physiol Regul Integr Comp Physiol. 2021. PMID: 33146554 Free PMC article.
-
MiR-590-3p and its targets VEGF, PIGF, and MMP9 in early, middle, and late pregnancy: their longitudinal changes and correlations with risk of fetal growth restriction.Ir J Med Sci. 2022 Jun;191(3):1251-1257. doi: 10.1007/s11845-021-02664-6. Epub 2021 Jun 22. Ir J Med Sci. 2022. PMID: 34159524
-
Fetal adrenal demedullation lowers circulating norepinephrine and attenuates growth restriction but not reduction of endocrine cell mass in an ovine model of intrauterine growth restriction.Nutrients. 2015 Jan 9;7(1):500-16. doi: 10.3390/nu7010500. Nutrients. 2015. PMID: 25584967 Free PMC article.
References
-
- Adamson SL. Arterial pressure, vascular input impedance, and resistance as determinants of pulsatile blood flow in the umbilical artery. Eur J Obstet Gynecol Reprod Biol. 1999;84:119–125. - PubMed
-
- Ahmed A, Dunk C, Ahmad S, Khaliq A. Regulation of placental vascular endothelial growth factor (VEGF) and placenta growth factor (PIGF) and soluble Flt-1 by oxygen-a review. Placenta. 2000;21(suppl A):S16–S24. - PubMed
-
- Ahmed A, Perkins J. Angiogenesis and intrauterine growth restriction. Best Pract Res Clin Obstet Gynaecol. 2000;14:981–998. - PubMed
-
- Ali KZ, Burton GJ, Morad N, Ali ME. Does hypercapillarization influence the branching pattern of terminal villi in the human placenta at high altitude. Placenta. 1996;17:677–682. - PubMed
-
- Barbera A, Jones OW, Zerbe GO, Hobbins JC, Battaglia PC, Meschia G. Early ultrasonographic detection of fetal retardation in an ovine model of placental insufficiency. Am J Obstet Gynecol. 1995;173:1071–1074. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous