

White matter injury in the premature infant: a comparison between serial cranial sonographic and MR findings at term
- PMID: 12748075
- PMCID: PMC7975772
White matter injury in the premature infant: a comparison between serial cranial sonographic and MR findings at term
Abstract
Background and purpose: The accuracy of cranial sonography (US) in characterizing white matter (WM) injury in the premature infant is unclear. This study was aimed to assess the sensitivity and specificity of serial cranial US during the first 6 weeks of life in comparison to MR imaging at term (week of expected delivery) in characterizing the presence of WM injury in a cohort of 96 very low birth weight (VLBW) infants.
Method: A blinded investigator reviewed serial cranial sonograms for the presence of WM echolucency and echodensity, including its duration and extent. These abnormalities were compared with a second independent investigator's evaluation to determine the sensitivity and specificity of cranial WM abnormalities at US.
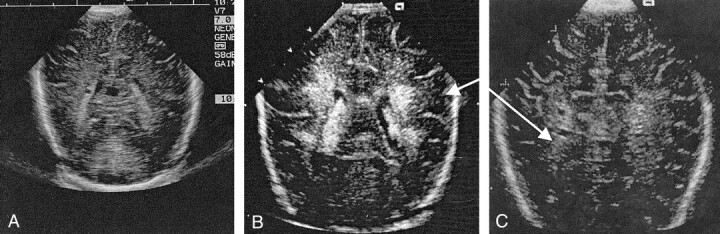
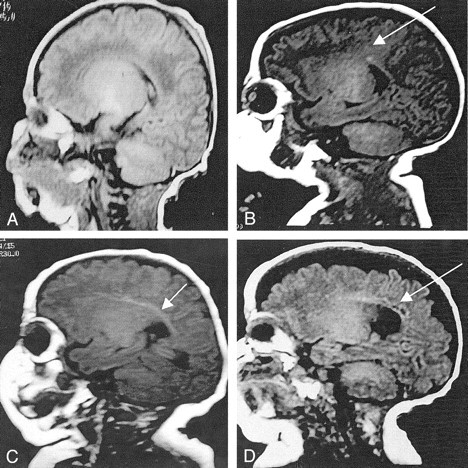
Results: The presence of prolonged echodensity (>7 days) in the WM on neonatal cranial sonograms demonstrated low sensitivity (26%) and a low positive predictive value (36%) for the presence of noncystic WM injury, as detected on MR images at term. Extensive cystic lesions detected on MR images were all identified during earlier cranial US.
Conclusion: Neonatal cranial US of the VLBW infant demonstrates high reliability in the detection of cystic WM injury but has significant limitations in the demonstration of noncystic WM injury. This deficiency of neonatal cranial US is important, because noncystic WM injury is considerably more common than cystic WM injury.
Figures
References
-
- Volpe JJ. Neurology of the Newborn. 4th ed. Philadelphia: WB Saunders,2001
-
- Hope PL, Gould SJ, Howard S, Hamilton PA, Costello AM, Reynolds EO. Precision of ultrasound diagnosis of pathologically verified lesions in the brains of very preterm infants. Dev Med Child Neurol 1988;30:457–471 - PubMed
-
- Paneth N, Rudelli R, Monte W, et al. White matter necrosis in very low birth weight infants: neuropathologic and ultrasonographic findings in infants surviving six days or longer. J Pediatr 1990;116:975–984 - PubMed
-
- Carson SC, Hertzberg BS, Bowie JD, Burger PC. Value of sonography in the diagnosis of intracranial hemorrhage and periventricular leukomalacia: A postmortem study of 35 cases. Am J Neuroradiol 1990;155:595–601 - PubMed
-
- Adcock LM, Moore PJ, Schlesinger AE, Armstrong DL. Correlation of ultrasound with postmortem neuropathologic studies in neonates. Pediatr Neurol 1998;19:263–271 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical