

Measurement of cerebral blood flow in chronic carotid occlusive disease: comparison of dynamic susceptibility contrast perfusion MR imaging with positron emission tomography
- PMID: 12748086
- PMCID: PMC7975791
Measurement of cerebral blood flow in chronic carotid occlusive disease: comparison of dynamic susceptibility contrast perfusion MR imaging with positron emission tomography
Abstract
Background and purpose: Our purpose was to evaluate the accuracy of cerebral blood flow (CBF) measurements obtained by using dynamic susceptibility contrast-enhanced MR imaging, including the influence of arterial input function (AIF) selection, compared with those obtained by using [(15)O]-H(2)O positron emission tomography (PET) for patients with chronic carotid occlusion.
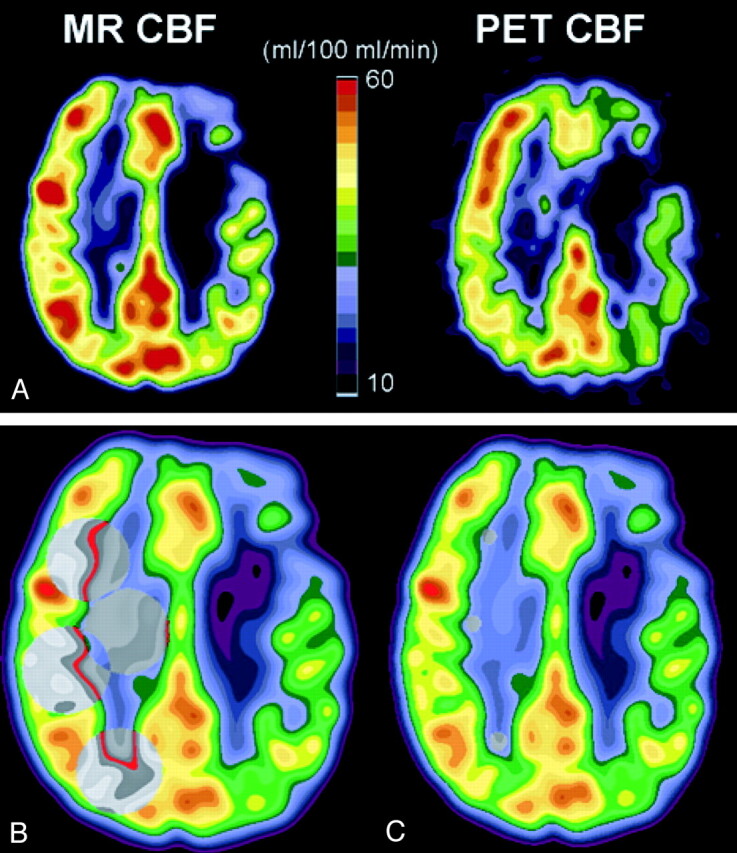
Methods: MR images and PET scans were obtained of seven patients with unilateral carotid occlusion and were co-registered for region of interest analysis. PET CBF maps were generated by using the autoradiographic method. MR imaging CBF maps were calculated by deconvolution of the susceptibility time curve with a proximal middle cerebral artery AIF and were converted to absolute flow rates either by assuming a constant contralateral white matter CBF value of 22 mL/100 mL/min or by using individually determined PET white matter CBF values.
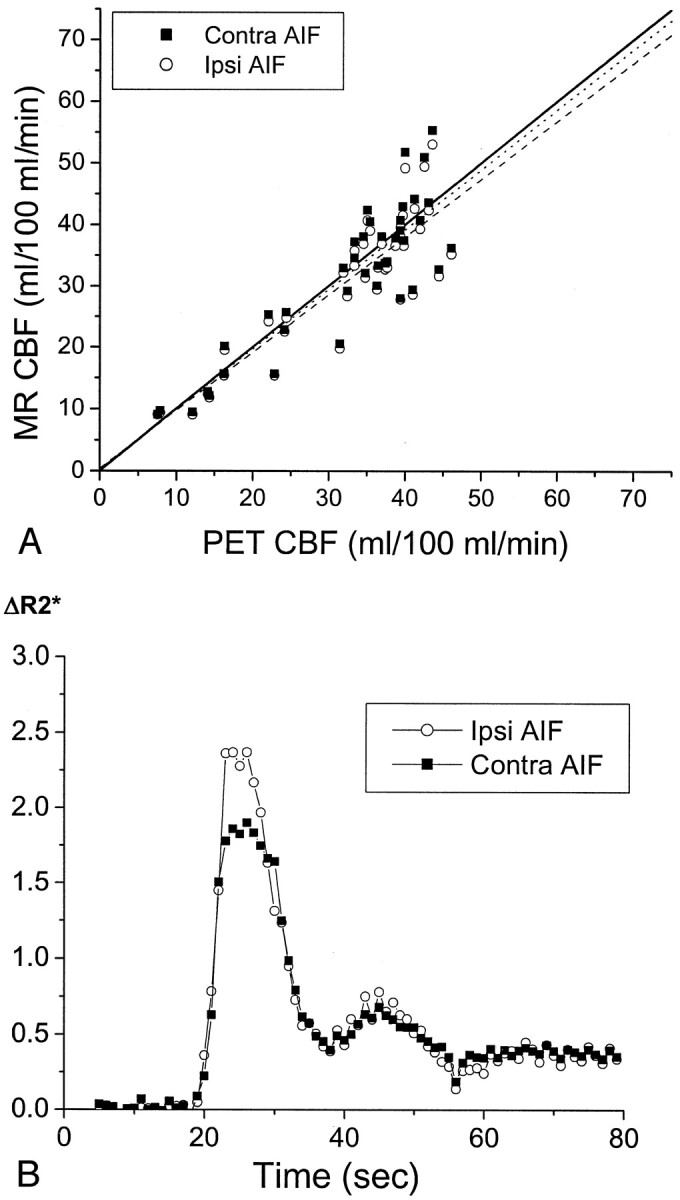
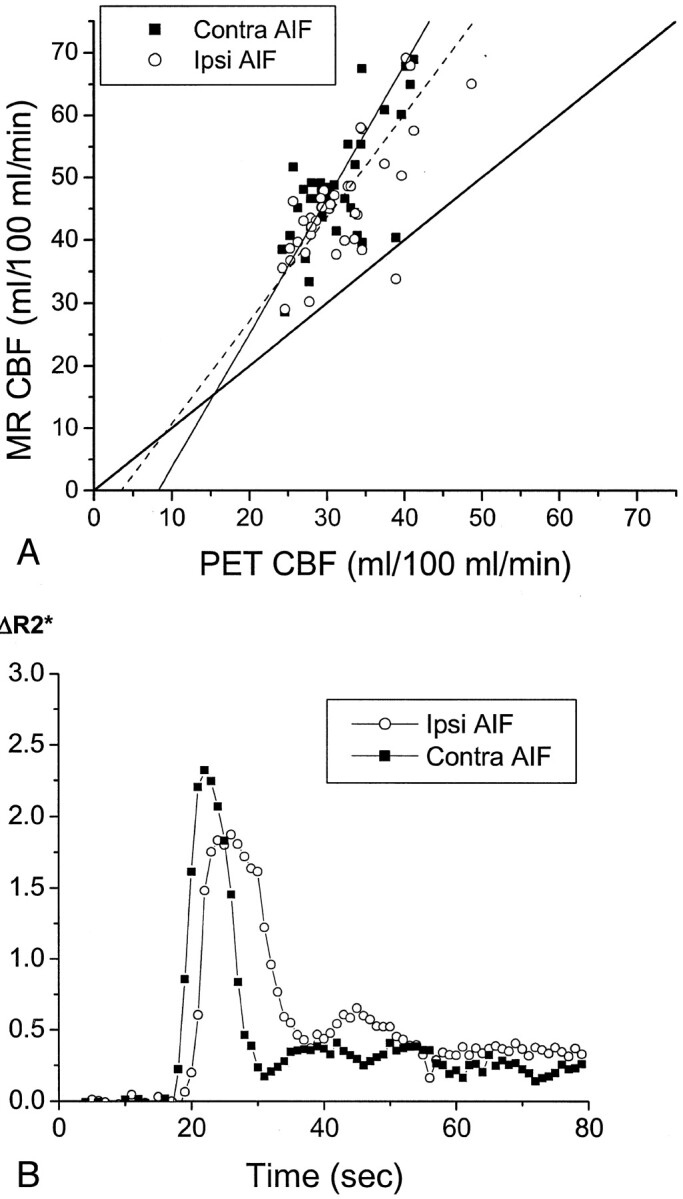
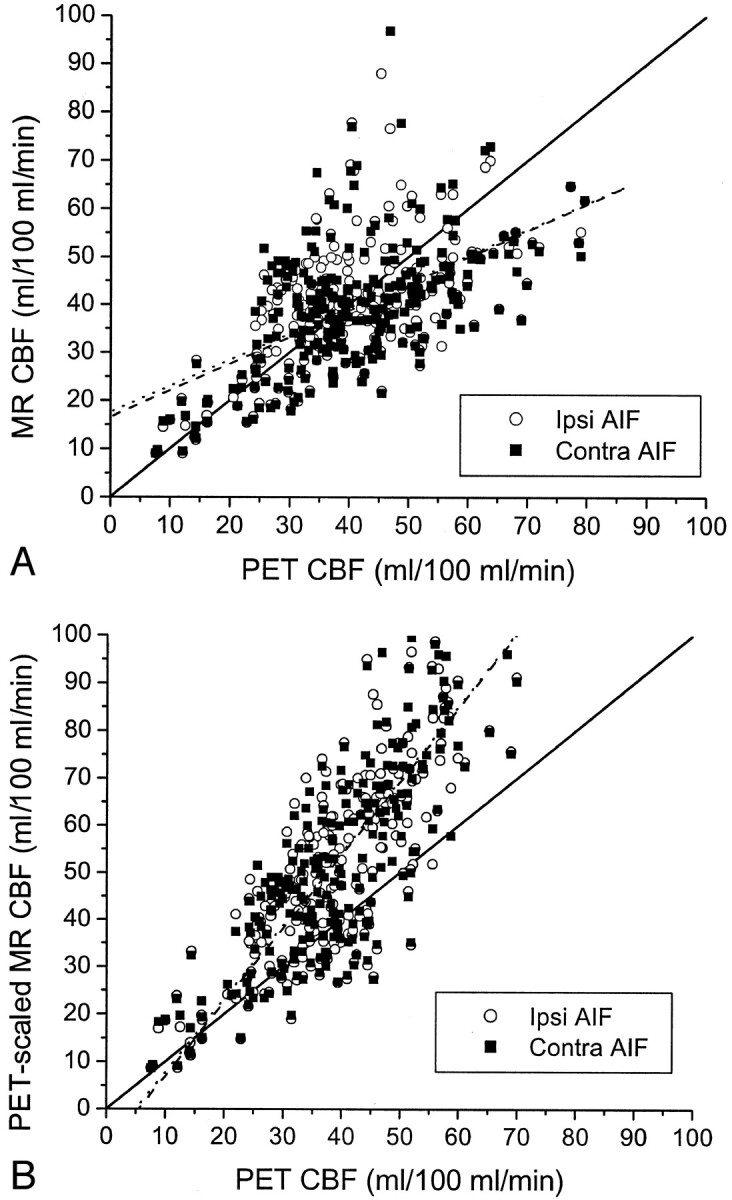
Results: Although CBF values measured by PET and MR imaging were positively correlated for every patient, the slopes and y intercepts of the regression lines varied widely among patients. The correlation was better when individual white matter CBF values measured by PET were used to scale the white matter CBF values measured by MR imaging (r = 0.84, P <.0001) than when constant contralateral CBF values were assumed (r = 0.54, P <.0001). The choice of AIF ipsilateral or contralateral to the occluded carotid artery made no statistically significant difference (P >.05) to the correlation coefficient, slope, or y intercept of the MR imaging versus PET CBF regressions for six of the seven patients.
Conclusion: Although linearly correlated with CBF values measured by PET, dynamic susceptibility contrast-enhanced MR imaging was not accurate for measuring absolute CBF values. AIF selection relative to the side of carotid occlusion did not significantly affect calculated MR imaging CBF values for six of the seven patients.
Figures
References
-
- Sorensen AG, Copen WA, Ostergaard L, et al. Hyperacute stroke: simultaneous measurement of relative cerebral blood volume, relative cerebral blood flow, and mean tissue transit time. Radiology 1999;210:519–527 - PubMed
-
- Knopp EA, Cha S, Johnson G, et al. Glial neoplasms: dynamic contrast-enhanced T2*-weighted MR imaging. Radiology 1999;211:791–798 - PubMed
-
- Ernst TM, Chang L, Witt MD, et al. Cerebral toxoplasmosis and lymphoma in AIDS: perfusion MR imaging experience in 13 patients. Radiology 1998;208:663–669 - PubMed
-
- Rempp KA, Brix G, Wenz F, Becker CR, Guckel F, Lorenz WJ. Quantification of regional cerebral blood flow and volume with dynamic susceptibility contrast-enhanced MR imaging. Radiology 1994;193:637–641 - PubMed
-
- Ostergaard L, Weisskoff RM, Chesler DA, Gyldensted C, Rosen BR. High resolution measurement of cerebral blood flow using intravascular tracer bolus passages: part I. mathematical approach and statistical analysis. Magn Reson Med 1996;36:715–725 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical