

Stenting of the ductus arteriosus and banding of the pulmonary arteries: basis for various surgical strategies in newborns with multiple left heart obstructive lesions
- PMID: 12748222
- PMCID: PMC1767699
- DOI: 10.1136/heart.89.6.645
Stenting of the ductus arteriosus and banding of the pulmonary arteries: basis for various surgical strategies in newborns with multiple left heart obstructive lesions
Abstract
Objective: To present an institutional experience with stent placement in the arterial duct combined with bilateral banding of the pulmonary artery branches as a basis for various surgical strategies in newborns with hypoplastic left heart obstructive lesions.
Design: Observational study.
Setting: Paediatric heart centre in a university hospital.
Patients: 20 newborns with various forms of left heart obstructive lesions and duct dependent systemic blood flow.
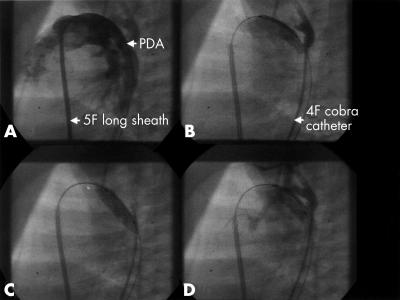
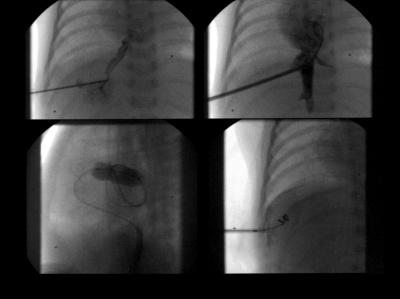
Interventions: Patients underwent percutaneous ductal stenting and surgical bilateral pulmonary artery banding. Atrial septotomy by balloon dilatation was performed as required, in one premature baby by the transhepatic approach.
Main outcome measures: Survival; numbers of and reasons for palliative and corrective cardiac surgery.
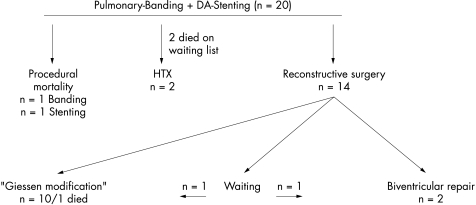
Results: One patient died immediately after percutaneous ductal stenting. One patient died in connection with the surgical approach of bilateral pulmonary banding. Stent and ductal patency were achieved for up to 331 days. Two patients underwent heart transplantation and two patients died on the waiting list. Ten patients had a palliative one stage procedure with reconstruction of the aortic arch and bidirectional cavopulmonary connection at the age of 3.5-6 months. There was one death. One patient is still awaiting this approach. Two patients received biventricular repair. In one, biventricular repair will soon be provided.
Conclusions: Stenting the arterial duct combined with bilateral pulmonary artery banding in newborns with hypoplastic left heart or multiple left heart obstructive lesions allows a broad variation of surgical strategies depending on morphological findings, postnatal clinical conditions, and potential ventricular growth.
Figures
Similar articles
-
A review of ductal stenting in hypoplastic left heart syndrome: bridge to transplantation and hybrid stage I palliation.Pediatr Cardiol. 2008 Mar;29(2):251-7. doi: 10.1007/s00246-007-0012-0. Epub 2007 Oct 3. Pediatr Cardiol. 2008. PMID: 17914595 Review.
-
Hybrid transcatheter-surgical palliation: basis for univentricular or biventricular repair: the Giessen experience.Pediatr Cardiol. 2007 Mar-Apr;28(2):79-87. doi: 10.1007/s00246-006-1444-7. Epub 2007 Feb 15. Pediatr Cardiol. 2007. PMID: 17487538
-
Stenting of the arterial duct and banding of the pulmonary arteries: basis for combined Norwood stage I and II repair in hypoplastic left heart.Circulation. 2002 Mar 5;105(9):1099-103. doi: 10.1161/hc0902.104709. Circulation. 2002. PMID: 11877362
-
Bilateral pulmonary artery banding for resuscitation in high-risk, single-ventricle neonates and infants: a single-center experience.J Thorac Cardiovasc Surg. 2013 Jan;145(1):206-13; discussion 213-4. doi: 10.1016/j.jtcvs.2012.09.063. J Thorac Cardiovasc Surg. 2013. PMID: 23244255
-
Hybrid palliation in hypoplastic left heart syndrome.Curr Opin Cardiol. 2007 Mar;22(2):55-9. doi: 10.1097/HCO.0b013e328014d945. Curr Opin Cardiol. 2007. PMID: 17284980 Review.
Cited by
-
Hypoplastic Left Heart: Stage-I Will be Performed Interventionally, Soon.Pediatr Cardiol. 2021 Apr;42(4):727-735. doi: 10.1007/s00246-021-02597-y. Epub 2021 Apr 19. Pediatr Cardiol. 2021. PMID: 33871681 Free PMC article. Review.
-
A review of ductal stenting in hypoplastic left heart syndrome: bridge to transplantation and hybrid stage I palliation.Pediatr Cardiol. 2008 Mar;29(2):251-7. doi: 10.1007/s00246-007-0012-0. Epub 2007 Oct 3. Pediatr Cardiol. 2008. PMID: 17914595 Review.
-
Pitfalls in hybrid procedures in newborns with left-sided obstructive lesions and duct-dependent systemic flow: single-center experience.Kardiochir Torakochirurgia Pol. 2025 Jun 24;22(2):79-87. doi: 10.5114/kitp.2025.152331. eCollection 2025 Jun. Kardiochir Torakochirurgia Pol. 2025. PMID: 40718664 Free PMC article.
-
Hypoplastic left heart syndrome: current perspectives.Transl Pediatr. 2016 Jul;5(3):142-147. doi: 10.21037/tp.2016.05.04. Transl Pediatr. 2016. PMID: 27709095 Free PMC article. Review.
-
Risk-stratified approach to hybrid transcatheter-surgical palliation of hypoplastic left heart syndrome.Pediatr Cardiol. 2006 Jan-Feb;27(1):91-95. doi: 10.1007/s00246-005-1028-y. Pediatr Cardiol. 2006. PMID: 16132295
References
-
- Bauer J, Thul J, Krämer U, et al. Heart transplantation in children and infants: short-term outcome and long-term follow-up. Pediatr Transplant 2001;5:457–62. - PubMed
-
- Ishino K, Stümper O, De Giovanni JV, et al. The modified Norwood procedure for hypoplastic left heart syndrome: early to intermediate results of 120 patients with particular reference to aortic arch repair. J Thorac Cardiovasc Surg 1999;117:920–30. - PubMed
-
- Thies WR, Breymann T, Cherlet E, et al. Anatomical and functional hypoplastic left heart syndrome and its surgical therapy by Norwood and Fontan operation. Z Kardiol 1997;86:505–13. - PubMed
-
- Mahle WT, Spray TL, Gaynor JW, et al. Unexpected death after reconstructive surgery for hypoplastic left heart syndrome. Ann Thorac Surg 2001;71:61–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources