

Review
doi: 10.1136/bmj.326.7398.1080.
ABC of interventional cardiology: percutaneous coronary intervention. I: history and development
Affiliations
- PMID: 12750213
- PMCID: PMC1125993
- DOI: 10.1136/bmj.326.7398.1080
Item in Clipboard
Review
ABC of interventional cardiology: percutaneous coronary intervention. I: history and development
BMJ.
.
No abstract available
Figures
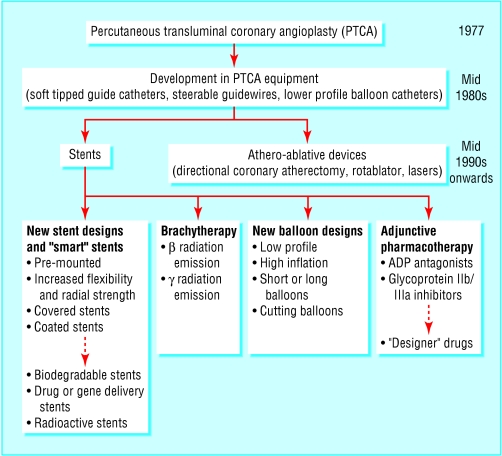
Major milestones in percutaneous coronary intervention
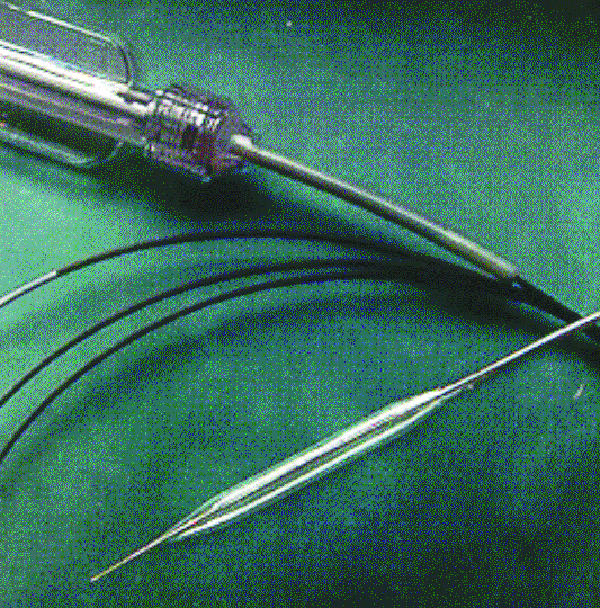
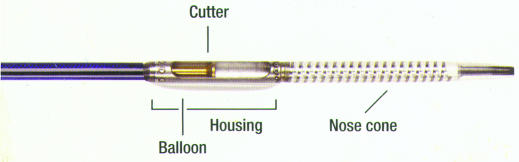
Modern balloon catheter: its low profile facilitates lesion crossing,
the flexible shaft allows tracking down tortuous vessels, and the balloon can
be inflated to high pressures without distortion or rupture
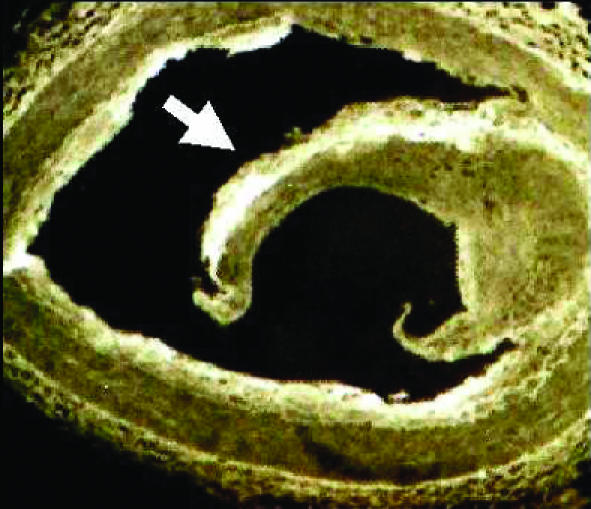
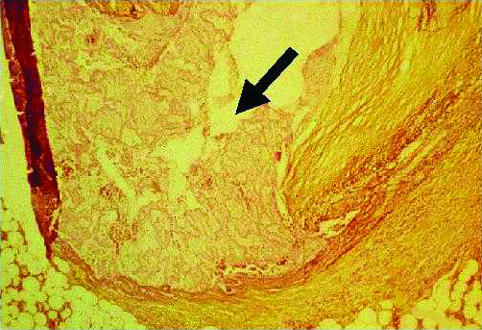
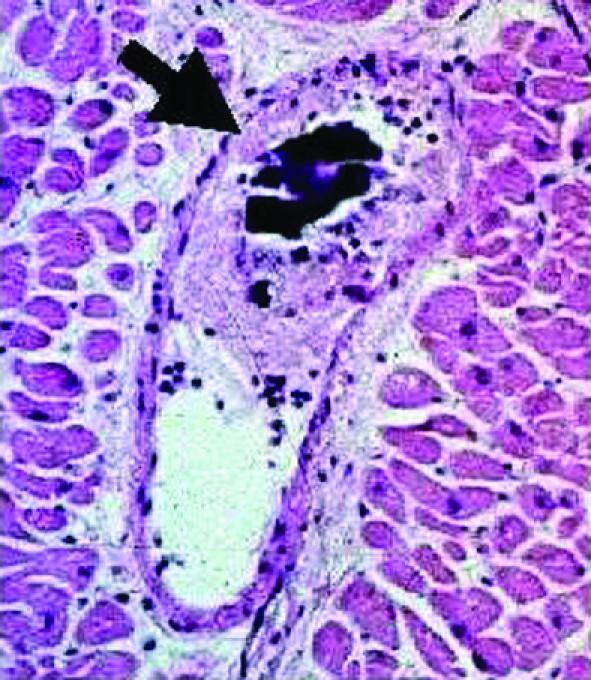
Micrographs showing arterial barotrauma caused by coronary angioplasty.
Top left: coronary arterial dissection with large flap. Top right: deep
fissuring within coronary artery wall atheroma. Bottom: fragmented plaque
tissue (dark central calcific plaque surrounded by fibrin and platelet-rich
thrombus), which may embolise in distal arterioles to cause infarction, and
intramural and perivascular haemorrhage (bottom)
Micrographs showing arterial barotrauma caused by coronary angioplasty.
Top left: coronary arterial dissection with large flap. Top right: deep
fissuring within coronary artery wall atheroma. Bottom: fragmented plaque
tissue (dark central calcific plaque surrounded by fibrin and platelet-rich
thrombus), which may embolise in distal arterioles to cause infarction, and
intramural and perivascular haemorrhage (bottom)
Micrographs showing arterial barotrauma caused by coronary angioplasty.
Top left: coronary arterial dissection with large flap. Top right: deep
fissuring within coronary artery wall atheroma. Bottom: fragmented plaque
tissue (dark central calcific plaque surrounded by fibrin and platelet-rich
thrombus), which may embolise in distal arterioles to cause infarction, and
intramural and perivascular haemorrhage (bottom)
Tools for coronary atherectomy. Top: the Simpson atherocath has a cutter
in a hollow cylindrical housing. The cutter rotates at 2000 rpm, and excised
atheromatous tissue is pushed into the distal nose cone. Left: the Rotablator
burr is coated with 10 μm diamond chips to create an abrasive surface. The
burr, connected to a drive shaft and a turbine powered by compressed air,
rotates at speeds up to 200 000 rpm

Tools for coronary atherectomy. Top: the Simpson atherocath has a cutter
in a hollow cylindrical housing. The cutter rotates at 2000 rpm, and excised
atheromatous tissue is pushed into the distal nose cone. Left: the Rotablator
burr is coated with 10 μm diamond chips to create an abrasive surface. The
burr, connected to a drive shaft and a turbine powered by compressed air,
rotates at speeds up to 200 000 rpm

Coronary stents. Top: Guidant Zeta stent. Middle: BiodivYsio AS stent
coated with phosphorylcholine, a synthetic copy of the outer membrane of red
blood cells, which improves haemocompatibility and reduces thrombosis. Bottom:
the Jomed JOSTENT coronary stent graft consists of a layer of PTFE
(polytetrafluoroethylene) sandwiched between two stents and is useful in
sealing perforations, aneurysms, and fistulae

Coronary stents. Top: Guidant Zeta stent. Middle: BiodivYsio AS stent
coated with phosphorylcholine, a synthetic copy of the outer membrane of red
blood cells, which improves haemocompatibility and reduces thrombosis. Bottom:
the Jomed JOSTENT coronary stent graft consists of a layer of PTFE
(polytetrafluoroethylene) sandwiched between two stents and is useful in
sealing perforations, aneurysms, and fistulae

Coronary stents. Top: Guidant Zeta stent. Middle: BiodivYsio AS stent
coated with phosphorylcholine, a synthetic copy of the outer membrane of red
blood cells, which improves haemocompatibility and reduces thrombosis. Bottom:
the Jomed JOSTENT coronary stent graft consists of a layer of PTFE
(polytetrafluoroethylene) sandwiched between two stents and is useful in
sealing perforations, aneurysms, and fistulae
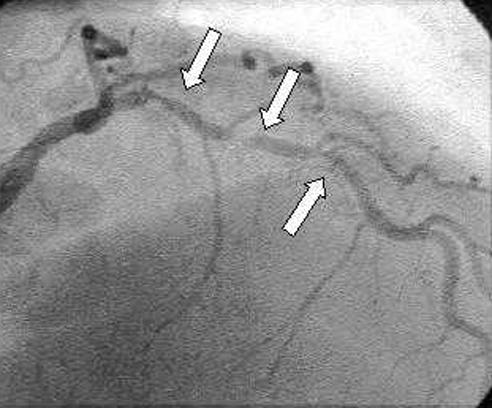
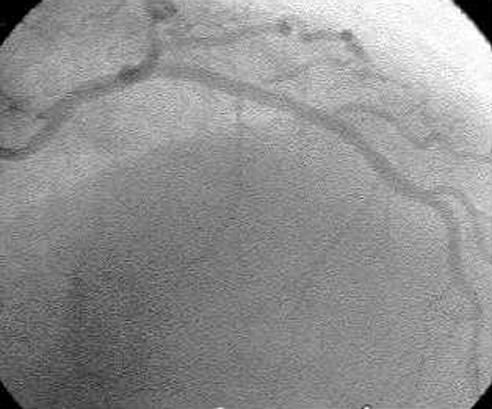
Coronary angiogram showing three lesions (arrows) affecting the left
anterior descending artery (top left). The lesions are stented without
pre-dilatation (top right), with good results (bottom)

Coronary angiogram showing three lesions (arrows) affecting the left
anterior descending artery (top left). The lesions are stented without
pre-dilatation (top right), with good results (bottom)
Coronary angiogram showing three lesions (arrows) affecting the left
anterior descending artery (top left). The lesions are stented without
pre-dilatation (top right), with good results (bottom)
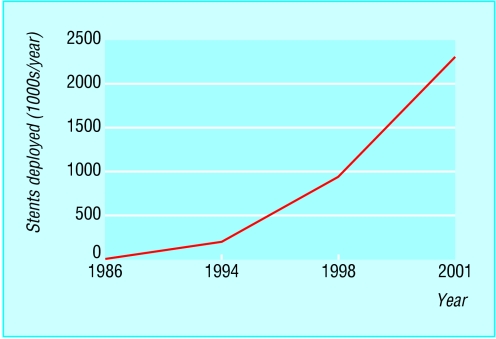
Exponential increase in use of intracoronary stents since 1986. In 2001,
2.3 million stents were implanted (more than double the 1998 rate)
References
-
- Gruentzig AR. Transluminal dilatation of coronary artery stenosis. Lancet 1978;1: 263. - PubMed
-
- Smith SC Jr, Dove JT, Jacobs AK, Kennedy JW, Kereiakes D, Kern MJ, et al. ACC/AHA guidelines of percutaneous coronary interventions (revision of the 1993 PTCA guidelines)-executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty). J Am Coll Cardiol 2001;37: 2215-39 - PubMed
-
- Meyer BJ, Meier B. Percutaneous transluminal coronary angioplasty of single or multivessel disease and chronic total occlusions. In: Grech ED, Ramsdale DR, eds. Practical interventional cardiology. 2nd ed. London: Martin Dunitz, 2002: 35-54
-
- Costa MA, Foley DP, Serruys PW. Restenosis: the problem and how to deal with it. In: Grech ED, Ramsdale DR, eds. Practical interventional cardiology. 2nd ed. London: Martin Dunitz, 2002: 279-94
-
- Topol EJ, Serruys PW. Frontiers in interventional cardiology. Circulation 1998;98: 1802-20 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical