

Bochdalek diaphragmatic hernia: not only a neonatal disease
- PMID: 12765926
- PMCID: PMC1763105
- DOI: 10.1136/adc.88.6.532
Bochdalek diaphragmatic hernia: not only a neonatal disease
Abstract
Aims: To characterise the clinical manifestations of late presenting Bochdalek diaphragmatic hernia (DH), the incidence of misdiagnosis, and prognosis; and to explore the sequence of events that leads to this clinical picture.
Methods: Retrospective chart review. All children with Bochdalek DH were identified. Children 1 month of age and older at the time of diagnosis were included.
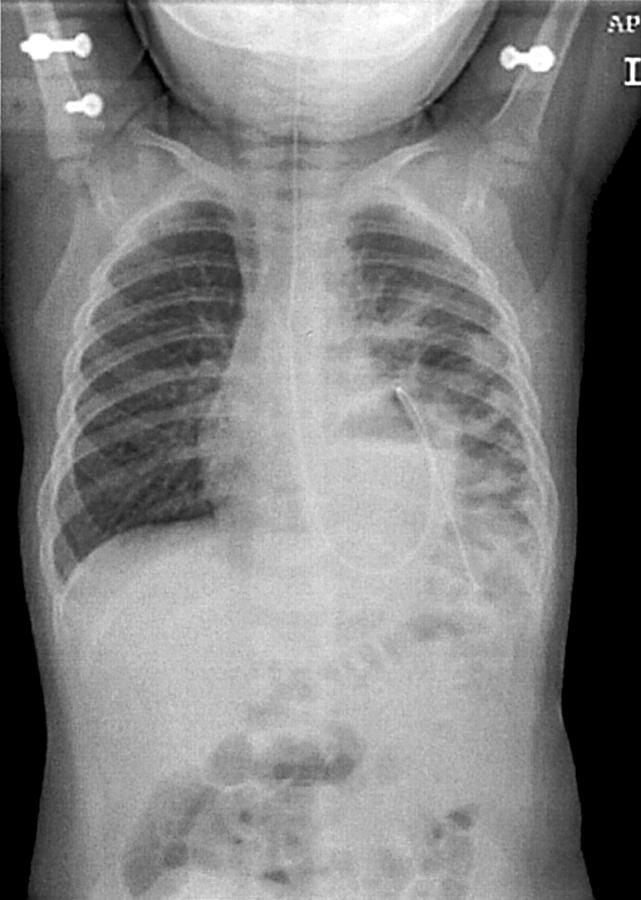
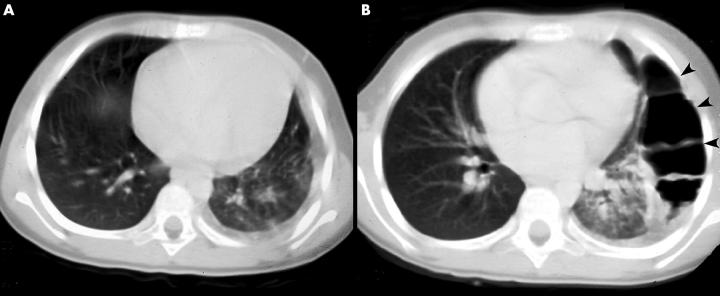
Results: Twenty two children with Bochdalek DH met the inclusion criteria. Three clinical presentations could be defined. Fourteen children presented with acute onset of symptoms, predominantly vomiting and respiratory distress. Four had chronic non-specific gastrointestinal or respiratory symptoms, and in four the DH was found incidentally. Although five children were initially misdiagnosed, in 20 children (91%) the correct diagnosis was made on x ray examination. One child experienced a complicated course when the x ray picture was misinterpreted as pneumothorax. All children had favourable outcome. Two children had previously normal chest imaging, suggesting acquired herniation. A large pleural effusion without DH in a 9.5 year old girl with an abdominal infection prior to presenting with herniation suggests a pre-existing defect in the diaphragm.
Conclusions: Late presenting Bochdalek DH can present with acute or chronic gastrointestinal, or less frequently, respiratory symptoms. It can also be found incidentally. Misdiagnosis can result in significant morbidity. Favourable outcome is expected when the correct diagnosis is made. The sequence of events is probably herniation of abdominal viscera through a pre-existing diaphragmatic defect. Although rare, DH should be considered in any child presenting with respiratory distress or with symptoms suggestive of gastrointestinal obstruction.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous