

Milk transfer and neonatal safety of tacrolimus
- PMID: 12773068
- PMCID: PMC3636979
- DOI: 10.1345/aph.1C312
Milk transfer and neonatal safety of tacrolimus
Abstract
Objective: To report the first case of tacrolimus measurement in human milk following maternal dosing in a woman who breast-fed while taking the medication.
Case report: A 32-year-old white woman who had taken tacrolimus 0.1 mg/kg/d throughout pregnancy contacted the Motherisk Program at 35 weeks' gestation inquiring about the safety of breast-feeding during maternal tacrolimus therapy. After benefit-risk assessment, the mother decided to breast-feed the baby.
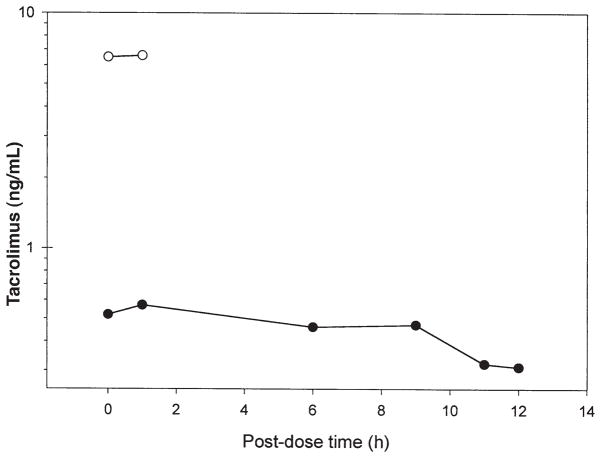
Methods: Manually expressed milk samples were collected over 12 hours following the first tacrolimus dose of the day; pre-dosing and 1-hour post-dosing blood concentrations were also determined. The samples were analyzed for tacrolimus by tandem-mass spectrometry. Breast milk and blood samples were collected at steady-state.
Results: The highest and mean concentrations of tacrolimus in milk were 0.57 and 0.429 ng/mL, respectively. From these measurements, the exclusively breast-fed infant would ingest, on average, 0.06 micro g/kg/d, which corresponds to 0.06% of the mother's weight-adjusted dose. Given the low oral bioavailability of tacrolimus, the maximum amount the baby would receive is 0.02% of the mother's weight-adjusted dose. The milk-to-blood ratios of tacrolimus at pre-dosing and 1-hour post-dosing concentrations were calculated to be 0.08 and 0.09, respectively. At 2.5 months of age, the infant was developing well both physically and neurologically.
Comment: This report is the first to measure tacrolimus concentrations in established human milk using tandem-mass spectrometry to detect drug while the infant was exclusively breast-fed by the mother, and in which the infant's growth and development were reported.
Conclusions: Our results suggest that maternal therapy with tacrolimus for liver transplant may be compatible with breast-feeding.
Figures
References
-
- Jusko WJ, Thomson AW, Fung J, McMaster P, Wong SH, Zylber-Katz E, et al. Consensus document: therapeutic monitoring of tacrolimus (FK-506) Ther Drug Monit. 1995;17:606–14. - PubMed
-
- Volosov A, Napoli KL, Soldin SJ. Simultaneous simple and fast quantification of three major immunosuppressants by liquid chromatography—tandem mass-spectrometry. Clin Biochem. 2001;34:285–90. - PubMed
-
- Product monograph: Prograf (tacrolimus) Markham, ON: Fujisawa Canada; 2001.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
