

A parsimonious explanation for intersecting perinatal mortality curves: understanding the effect of plurality and of parity
- PMID: 12780942
- PMCID: PMC166132
- DOI: 10.1186/1471-2393-3-3
A parsimonious explanation for intersecting perinatal mortality curves: understanding the effect of plurality and of parity
Abstract
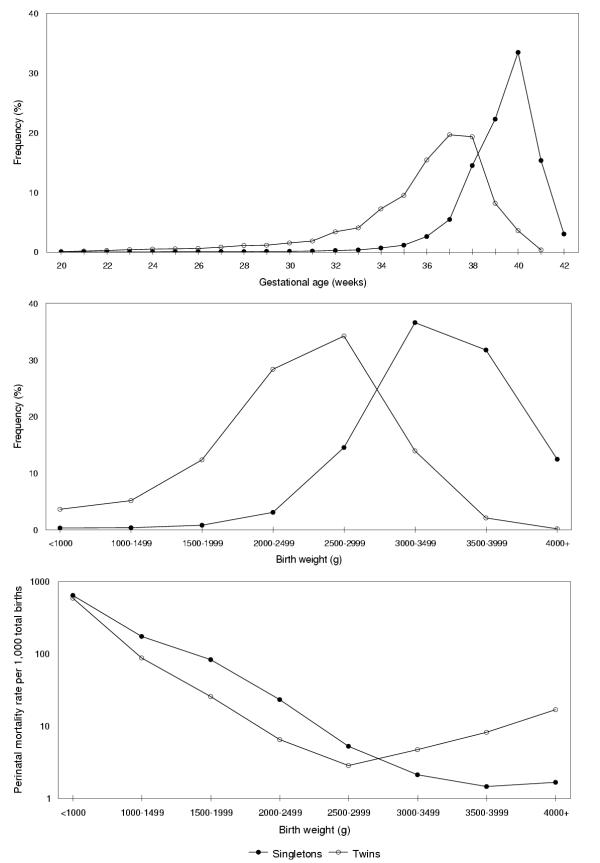
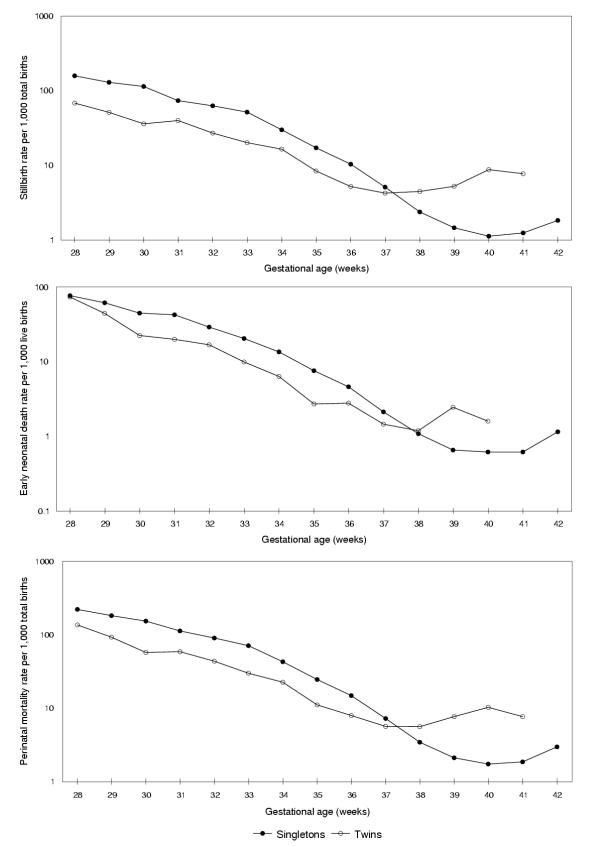
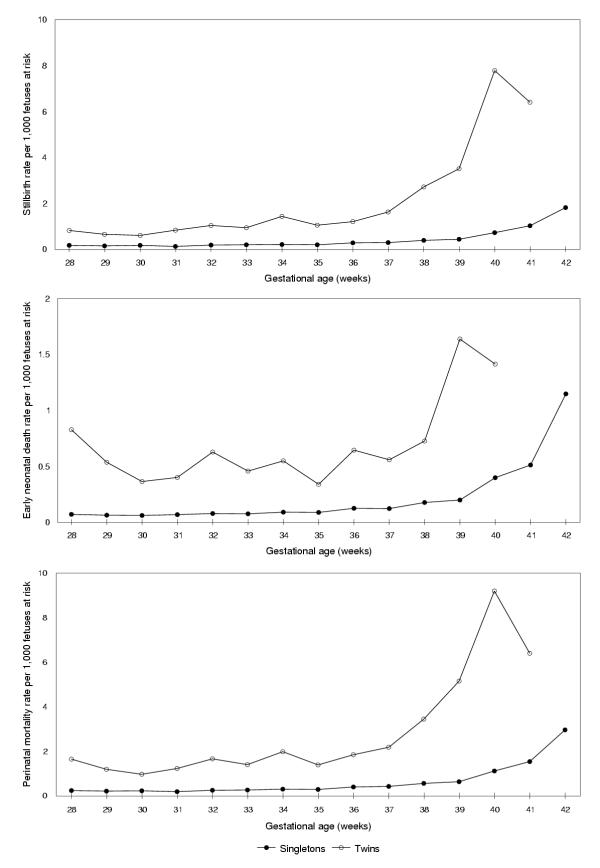
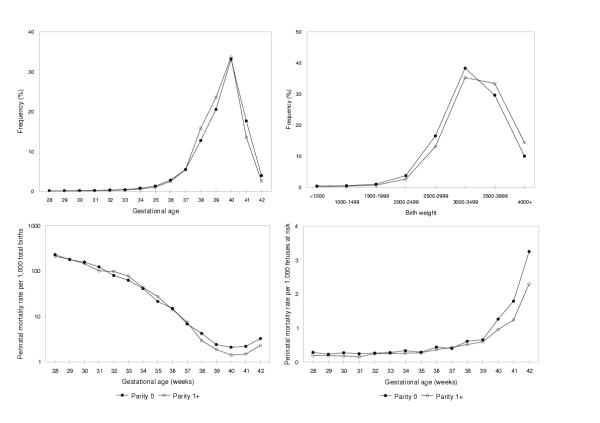
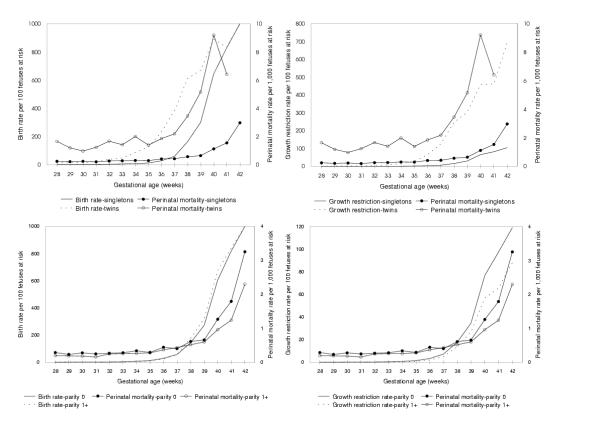
BACKGROUND: Birth weight- and gestational age-specific perinatal mortality curves intersect when compared across categories of maternal smoking, plurality, race and other factors. No simple explanation exists for this paradoxical observation. METHODS: We used data on all live births, stillbirths and infant deaths in Canada (1991-1997) to compare perinatal mortality rates among singleton and twin births, and among singleton births to nulliparous and parous women. Birth weight- and gestational age-specific perinatal mortality rates were first calculated by dividing the number of perinatal deaths at any given birth weight or gestational age by the number of total births at that birth weight or gestational age (conventional calculation). Gestational age-specific perinatal mortality rates were also calculated using the number of fetuses at risk of perinatal death at any given gestational age. RESULTS: Conventional perinatal mortality rates among twin births were lower than those among singletons at lower birth weights and earlier gestation ages, while the reverse was true at higher birth weights and later gestational ages. When perinatal mortality rates were based on fetuses at risk, however, twin births had consistently higher mortality rates than singletons at all gestational ages. A similar pattern emerged in contrasts of gestational age-specific perinatal mortality among singleton births to nulliparous and parous women. Increases in gestational age-specific rates of growth-restriction with advancing gestational age presaged rising rates of gestational age-specific perinatal mortality in both contrasts. CONCLUSIONS: The proper conceptualization of perinatal risk eliminates the mortality crossover paradox and provides new insights into perinatal health issues.
Figures
References
-
- Yerushalmy J. The relationship of parents' cigarette smoking to outcome of pregnancy – implications as to the problem of inferring causation from observed associations. Am J Epidemiol. 1971;93:443–456. - PubMed
-
- Meyer MB, Comstock GW. Maternal cigarette smoking and perinatal mortality. Am J Epidemiol. 1972;96:1–10. - PubMed
-
- Wilcox AJ, Russell IT. Birthweight and perinatal mortality: III. Towards a new method of analysis. Int J Epidemiol. 1986;15:188–196. - PubMed
-
- English PB, Eskenazi B. Reinterpreting the effects of maternal smoking on infant birthweight and perinatal mortality: a multivariate approach to birth weight standardization. Int J Epidemiol. 1992;21:1097–1105. - PubMed
LinkOut - more resources
Full Text Sources
