

A comparative study of vaginal misoprostol and intravenous oxytocin for induction of labour in women with intra uterine fetal death in Mulago Hospital, Uganda
- PMID: 12789117
- PMCID: PMC2141556
A comparative study of vaginal misoprostol and intravenous oxytocin for induction of labour in women with intra uterine fetal death in Mulago Hospital, Uganda
Abstract
Background: Intrauterine fetal death is a major problem in obstetrics particularly in developing countries such as Uganda. Induction of labour in cases of fetal death using the available method of oxytocin is often difficult, expensive and frustrating.
Objectives: To compare the effectiveness of vaginal misoprostol and intravenous oxytocin in induction of labour in women with intrauterine fetal death.
Methods: One hundred and twenty mothers were allocated in a randomised controlled way to one of the two induction groups. Oxytocin infusion was titrated based on patient response. The starting dose was 50 mcg (1/4 tablet) in misoprostol group and the dose was doubled every six hours till effective contractions were achieved. The two groups were compared for induction to delivery intervals, costs of the drugs and their safety during induction.
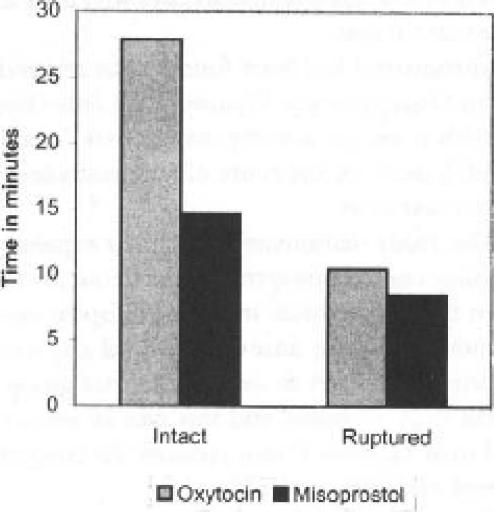
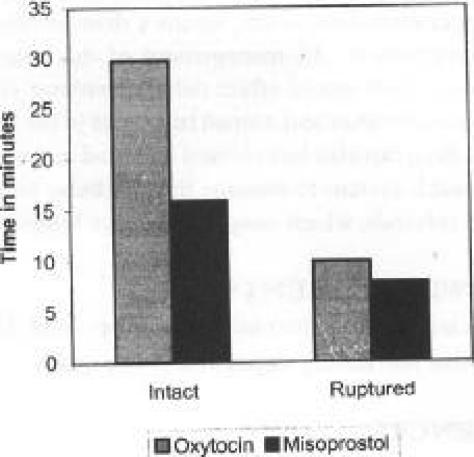
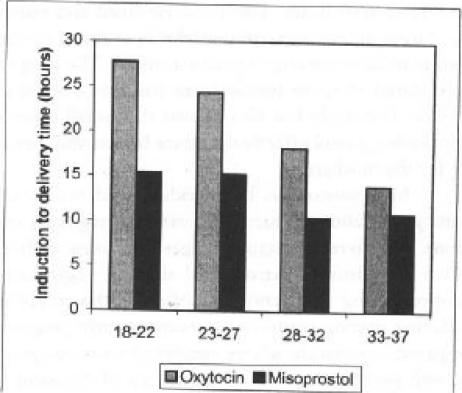
Results: The success rate within 48 hours of induction was 100% in the misoprostol group and 96.7% in oxytocin group. The mean induction to delivery time was significantly longer in the oxytocin group compared with the misoprostol group (23.3 versus 12.4 hours; p= 0.004). In the gestational age before 28 weeks, the induction to delivery interval in oxytocin group, was more than twice that used in misoprostol. However beyond 28 weeks, there was no significant difference. Women with intact membranes had induction to delivery interval of 27.9 hours in the oxytocin group and 14.7 hours in the misoprostol group (p=0.002). When the membranes were ruptured, the values were 10.5 and 8.5 hours respectively (p=0.6). The induction to delivery time in cases with Bishop's score < 6 was 29.8 hours in the oxytocin group and 15.9 hours in misoprostol group (p=0.001). The corresponding values for Bishop's scores > 6 were 10 and 7.9 hours respectively (p=0.6). The majority of patients in misoprostol group (62%), required less than one tablet for successful induction. Misoprostol was cheaper (0.65 US dollars than oxytocin (7.86 US dollars) Retained placenta occurred in only 3.3% of the patients in the misoprostol group. There were no cases of ruptured uterus in both groups.
Conclusion: Intravaginal misoprostol is more effective and cheaper than intravenous oxytocin for inducing labour in patients with intrauterine fetal death.
Figures
Comment in
-
Clarifying the role of misoprostol in obstetrics.Afr Health Sci. 2001 Dec;1(2):52-4. Afr Health Sci. 2001. PMID: 12789116 Free PMC article. No abstract available.
References
-
- Bugalho A, Bergstrom S. Induction of labour by vaginal misoprostol. Acta Obstet Gynecol Scand. 1999;78:653–654. - PubMed
-
- Bugalho A, Machungo F, Bique C. Induction of labour with intravaginal misoprostol in intrauterine fetal death. Am J Obstet Gynecol. 1994;171:538–541. - PubMed
-
- Choy-Hee I, Raynor BD. Misoprostol in induction of labour in women with prior Caesarean section. Am J Obstet Gynecol. 2000;182:S15. - PubMed
-
- Cunha M, Bugalho A, Bergstrom S, et al. Induction of labour by vaginal misoprostol in patients with previous caesarean delivery. Acta Obstet Gynecol Scand. 1999;78:653–654. - PubMed
-
- Danielsson KG, Marions L, Rodriguez A, et al. Comparison between oral and vaginal administration of misoprostol on uterine contractility. Obstet Gynecol. 1999;93:275–280. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources