

Severe sepsis: variation in resource and therapeutic modality use among academic centers
- PMID: 12793887
- PMCID: PMC270675
- DOI: 10.1186/cc2171
Severe sepsis: variation in resource and therapeutic modality use among academic centers
Abstract
Background: Treatment of severe sepsis is expensive, often encompassing a number of discretionary modalities. The objective of the present study was to assess intercenter variation in resource and therapeutic modality use in patients with severe sepsis.
Methods: We conducted a prospective cohort study of 1028 adult admissions with severe sepsis from a stratified random sample of patients admitted to eight academic tertiary care centers. The main outcome measures were length of stay (LOS; total LOS and LOS after onset of severe sepsis) and total hospital charges.
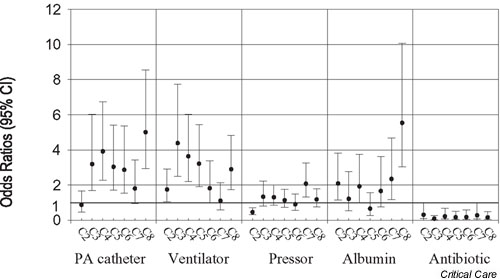
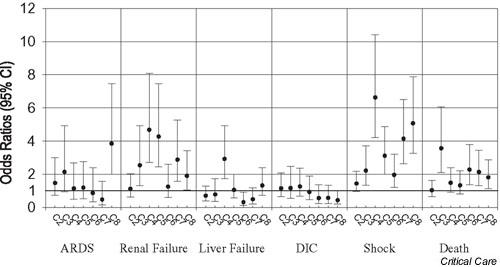
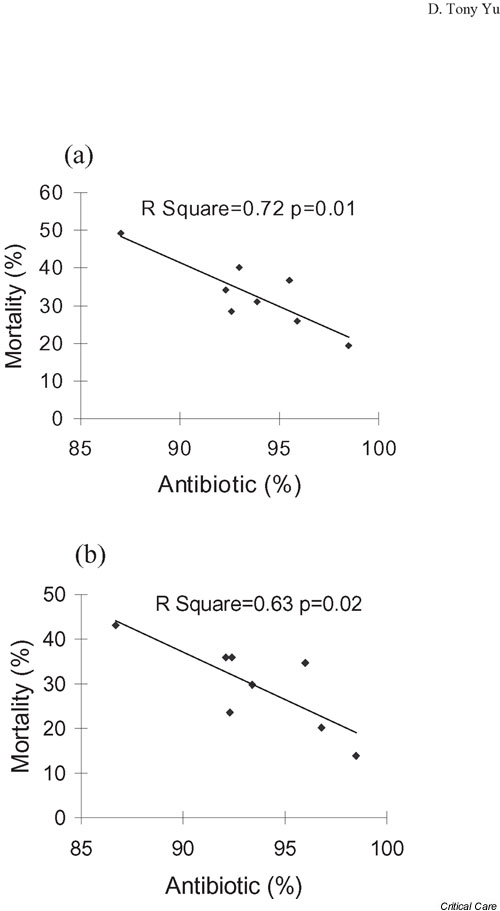
Results: The adjusted mean total hospital charges varied from 69 429 dollars to US237 898 dollars across centers, whereas the adjusted LOS after onset varied from 15.9 days to 24.2 days per admission. Treatments used frequently after the first onset of sepsis among patients with severe sepsis were pulmonary artery catheters (19.4%), ventilator support (21.8%), pressor support (45.8%) and albumin infusion (14.4%). Pulmonary artery catheter use, ventilator support and albumin infusion had moderate variation profiles, varying 3.2-fold to 4.9-fold, whereas the rate of pressor support varied only 1.92-fold across centers. Even after adjusting for age, sex, Charlson comorbidity score, discharge diagnosis-relative group weight, organ dysfunction and service at onset, the odds for using these therapeutic modalities still varied significantly across centers. Failure to start antibiotics within 24 hours was strongly correlated with a higher probability of 28-day mortality (r2 = 0.72).
Conclusion: These data demonstrate moderate but significant variation in resource use and use of technologies in treatment of severe sepsis among academic centers. Delay in antibiotic therapy was associated with worse outcome at the center level.
Figures
Comment in
-
Variation in sepsis care: a wake-up call.Crit Care. 2003 Jun;7(3):211-3. doi: 10.1186/cc2191. Epub 2003 May 1. Crit Care. 2003. PMID: 12793867 Free PMC article.
Similar articles
-
Relationship of pulmonary artery catheter use to mortality and resource utilization in patients with severe sepsis.Crit Care Med. 2003 Dec;31(12):2734-41. doi: 10.1097/01.CCM.0000098028.68323.64. Crit Care Med. 2003. PMID: 14668609
-
Resource utilization among patients with sepsis syndrome.Infect Control Hosp Epidemiol. 2003 Jan;24(1):62-70. doi: 10.1086/502117. Infect Control Hosp Epidemiol. 2003. PMID: 12558238
-
Frequency with which surgeons undertake pancreaticoduodenectomy determines length of stay, hospital charges, and in-hospital mortality.J Gastrointest Surg. 2001 Jan-Feb;5(1):21-6. doi: 10.1016/s1091-255x(01)80009-3. J Gastrointest Surg. 2001. PMID: 11309644
-
Comparison of Pediatric Severe Sepsis Managed in U.S. and European ICUs.Pediatr Crit Care Med. 2016 Jun;17(6):522-30. doi: 10.1097/PCC.0000000000000760. Pediatr Crit Care Med. 2016. PMID: 27124566 Free PMC article.
-
Epidemiology of sepsis: an update.Crit Care Med. 2001 Jul;29(7 Suppl):S109-16. doi: 10.1097/00003246-200107001-00035. Crit Care Med. 2001. PMID: 11445744 Review.
Cited by
-
Epidemiology of the Systemic Inflammatory Response Syndrome (SIRS) in the emergency department.West J Emerg Med. 2014 May;15(3):329-36. doi: 10.5811/westjem.2013.9.18064. Epub 2014 Feb 19. West J Emerg Med. 2014. PMID: 24868313 Free PMC article.
-
Variation in sepsis care: a wake-up call.Crit Care. 2003 Jun;7(3):211-3. doi: 10.1186/cc2191. Epub 2003 May 1. Crit Care. 2003. PMID: 12793867 Free PMC article.
-
Diagnosis and treatment of severe sepsis.Crit Care. 2007;11 Suppl 5(Suppl 5):S2. doi: 10.1186/cc6153. Crit Care. 2007. PMID: 18269689 Free PMC article. Review.
-
[The cost of sepsis].Anaesthesist. 2006 Jun;55 Suppl 1:36-42. doi: 10.1007/s00101-006-1039-y. Anaesthesist. 2006. PMID: 16685555 Review. German.
-
Incidence and outcome of sepsis in Japanese intensive care units: The Japanese nosocomial infection surveillance system.Environ Health Prev Med. 2006 Nov;11(6):298-303. doi: 10.1007/BF02898020. Environ Health Prev Med. 2006. PMID: 21432359 Free PMC article.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Niederman MS, Fein AM. Sepsis syndrome, the adult respiratory distress syndrome, and nosocomial pneumonia. A common clinical sequence. Clin Chest Med. 1990;11:633–656. - PubMed
-
- Rangel-Frausto MS, Pittet D, Costigan M, Hwang T, Davis CS, Wenzel RP. The natural history of the systemic inflammatory response syndrome (SIRS). A prospective study. JAMA. 1995;273:117–123. - PubMed
-
- Wenzel RP. Anti-endotoxin monoclonal antibodies: a second look. N Engl J Med. 1992;326:1151–1153. - PubMed
-
- Pittet D, Thievent B, Wenzel RP, Li N, Gurman G, Suter PM. Importance of pre-existing co-morbidities for prognosis of septicemia in critically ill patients. Intensive Care Med. 1993;19:265–272. - PubMed
