

Erythropoietin mimics the acute phase response in critical illness
- PMID: 12793888
- PMCID: PMC270680
- DOI: 10.1186/cc2185
Erythropoietin mimics the acute phase response in critical illness
Abstract
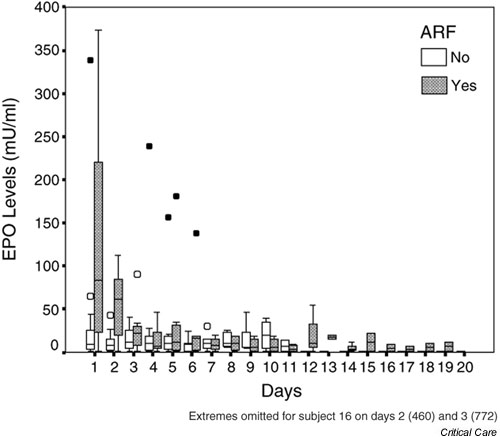
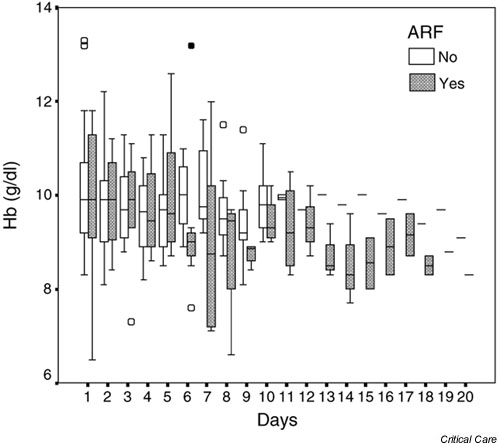
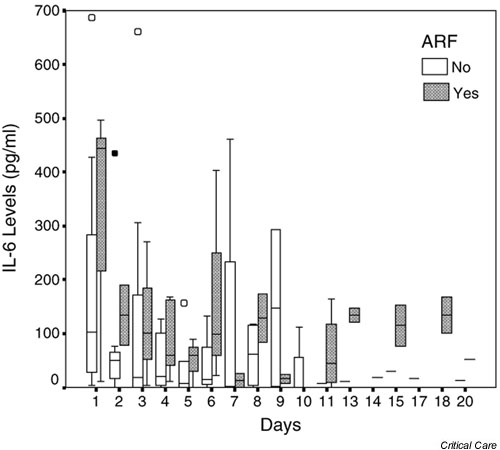
Background: In a prospective observational study, we examined the temporal relationships between serum erythropoietin (EPO) levels, haemoglobin concentration and the inflammatory response in critically ill patients with and without acute renal failure (ARF).
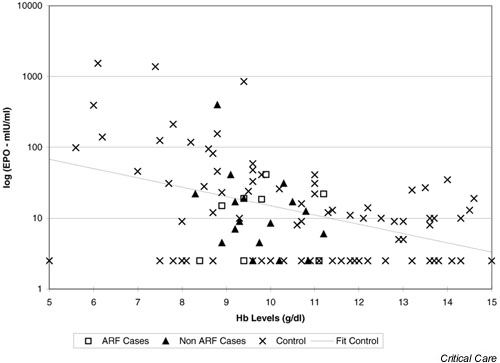
Patients and method: Twenty-five critically ill patients, from general and cardiac intensive care units (ICUs) in a university hospital, were studied. Eight had ARF and 17 had normal or mildly impaired renal function. The comparator group included 82 nonhospitalized patients with normal renal function and varying haemoglobin concentrations. In the patients, levels of haemoglobin, serum EPO, C-reactive protein, IL-1beta, IL-6, serum iron, ferritin, vitamin B12 and folate were measured, and Coombs test was performed from ICU admission until discharge or death. Concurrent EPO and haemoglobin levels were measured in the comparator group.
Results: EPO levels were initially high in patients with ARF, falling to normal or low levels by day 3. Thereafter, almost all ICU patients demonstrated normal or low EPO levels despite progressive anaemia. IL-6 exhibited a similar initial pattern, but levels remained elevated during the chronic phase of critical illness. IL-1beta was undetectable. Critically ill patients could not be distinguished from nonhospitalized anaemic patients on the basis of EPO levels.
Conclusion: EPO levels are markedly elevated in the initial phase of critical illness with ARF. In the chronic phase of critical illness, EPO levels are the same for patients with and those without ARF, and cannot be distinguished from noncritically ill patients with varying haemoglobin concentrations. Exogenous EPO therapy is unlikely to be effective in the first few days of critical illness.
Figures
References
-
- Von Ahsen N, Muller C, Serke S, Frei U, Eckardt K-U. Important role of nondiagnostic blood loss and blunted erythropoietic response in the anaemia of medical intensive care patients. Crit Care Med. 1999;27:2630–2639. - PubMed
-
- Hobisch-Hagen P, Wiedermann F, Mayr A, Fries D, Jelkmann W, Fuchs D, Hasibeder W, Mutz N, Klingler A, Schobersberger W. Blunted erythropoietic response to anemia in multiply traumatized patients. Crit Care Med. 2001;29:743–737. - PubMed
-
- Kraus P, Lipman J. Erythropoietin in a patient following multiple trauma. Anaesthesia. 1992;47:962–964. - PubMed
-
- Koestner JA, Nelson LD, Morris JA, Safcsak K. Use of recombinant human erythropoietin (r-HuEPO) in a Jehovah's witness refusing transfusion of blood products. J Trauma. 1990;30:1406–1408. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
